Arthroscopic Rotator Cuff Repair
Introduction
Many causative factors for rotator cuff disorders have been implicated, but pathogenesis remains controversial
Most common factors include age-related tendon degenerations, mechanical impingement, and changes in tendon vascularity
Natural history is recognized as a continuum, progressing from simple tendinopathy to partial- and full-thickness rotator cuff tears
Patient Selection

Figure 1Diagram depicts the treatment algorithm for shoulder pain consistent with rotator cuff pathology.
(Adapted with permission from Duquin TR, Sperling JW : Rotator cuff disorders, in Margheritini F, Rossi R, eds: Orthopaedic Sports Medicine: Principles and Practice. Milan, Italy, Springer-Verlag, 2011, pp 211-225.)
Patients must undergo thorough history and physical examination
Initial management consists of activity modification, NSAIDs, physical therapy, and possible corticosteroid injection (Figure 1)
Lack of improvement after 4 to 6 weeks indicates further investigation, including MRI
Preoperative Surgical Decision Making
Full-thickness or high-grade partial-thickness tears with associated pain and limited function despite an appropriate interval of nonsurgical management are candidates for arthroscopic repair
Primary indication is pain relief; improved strength and mobility are secondary
Contraindications
Absolute—Acute infections, significant glenohumeral arthritis, acromiohumeral arthropathy with fixed superior migration of the humeral head, inability to tolerate anesthesia, or inability to comply with postoperative rehabilitation
Relative—Chronic or recurrent tears, tears with massive size and/or significant retraction, poor tendon quality, poor muscle quality, profound motor dysfunction (clinical anterosuperior escape, chronic elevation or external rotation pseudoparalysis), multiple corticosteroid injections, medical comorbidities (diabetes mellitus, obesity), social factors (smoking status, Workers’ compensation claim), and advanced patient age
Preoperative Imaging
Radiography
True AP, scapular Y, and axillary views
Magnetic Resonance Imaging
T1- and T2-weighted images in coronal, sagittal, and oblique planes
Must include entire scapula on MRI to assess atrophy and fatty infiltration of rotator cuff
The tangent sign is used to quantify degree of supraspinatus atrophy
Ultrasonography
Acceptable alternative to MRI with near equivalent sensitivity and specificity
Extremely operator dependent
Procedure
Special Instruments/Equipment/Implants Required
30° arthroscope, fluid pump system, instruments for suture passing/retrieving/knot-tying, shavers and burrs, radiofrequency ablation wand. A variety of suture anchor types can be used for the repair
Authors’ preference—Biocomposite anchors, which are biodegradable with a lower risk of bone destruction
 | Video 26.1 Arthroscopic Rotator Cuff Repair. Thomas R. Duquin, MD; Donald W. Hohman, MD (30 min) |
Surgical Technique
Patient Positioning and Examination Under Anesthesia
Beach-chair or lateral decubitus position with careful positioning and wide prep and draping
Place surgical arm in articulated hydraulic arm holder
Perform examination under anesthesia on every shoulder to correlate preoperative pain and physical examination findings
Intra-articular Arthroscopy and Débridement
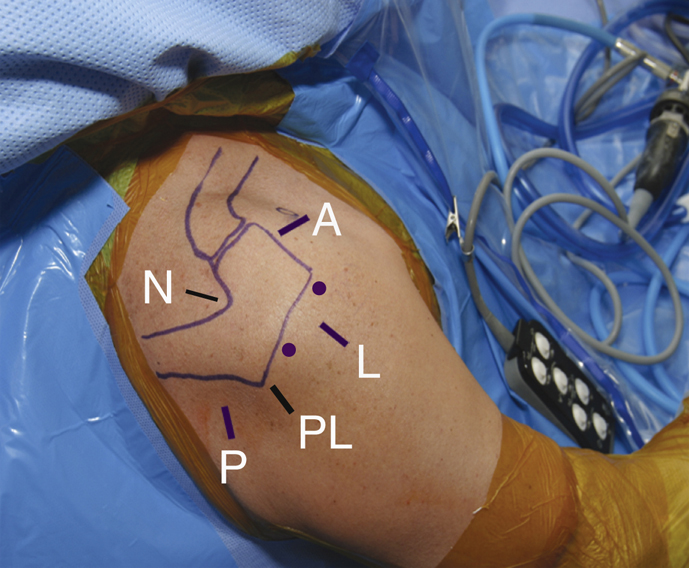
Figure 2Anatomic landmarks and the location of arthroscopic portals are marked on the skin. The circles represent stab incision locations for anchor introduction. A = anterior portal, L = lateral portal, N = Neviaser portal, P = posterior portal, PL = posterolateral portal.
TABLE 1
Tips for Portal Placement for Arthroscopic Rotator Cuff Repair
| Portal | Tip/Pearl | Location |
| Posterior portal | Provides best visualization of the shoulder joint; placement too far lateral should be avoided or joint visualization will be difficult | 1-3 cm distal and 1-2 cm medial to the posterolateral tip of the acromion |
| Anterior portal | Working portal for instruments and suture management; placed using the outside-in technique under arthroscopic visualization and spinal needle localization into the triangle formed by the labrum (medial border), biceps tendon (superior border), and subscapularis (inferior border) | Halfway between the acromioclavicular joint and the lateral aspect of the coracoid; pierces the anterior fibers of the deltoid and enters the joint in the interval between the supraspinatus and subscapularis |
| Lateral portal | Working portal for the subacromial space; used to visualize the subacromial space; if placed too posteriorly in a large or muscular patient, it will be difficult for the instruments to “turn the corner” to reach the anterior acromion. | Placed laterally, in line with the midclavicle and 2-3 cm lateral to its lateral edge |
| Posterolateral portal | Visualization of the subacromial space during rotator cuff repair | 1 cm distal to the posterolateral corner of the acromion |
| Neviaser | Working portal for the subacromial space; useful for suture passage in rotator cuff repair | Superomedial portal bordered by the clavicle, the acromioclavicular joint, and the spine of the scapula |
Identify and outline
The acromion, distal clavicle, and coracoid processes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


