CHAPTER 26 Arthroscopic Proximal Row Carpectomy
Introduction
Proximal row carpectomy is a motion-sparing salvage procedure that consists of excising the scaphoid, lunate, and capitate—thus converting a complex link joint into a simple hinge.1 Although the procedure has historically been criticized for loss of motion and strength, progressive radio capitate arthritis, and unpredictability of outcome, much of this criticism has been anecdotal.2 Recent studies, including three series with a minimum of nine years of follow-up, have demonstrated that proximal row carpectomy is as reliable a procedure as complex reconstructions and other salvage surgeries.3–16 The advantages of proximal row carpectomy include preservation of a functional arc of motion, satisfactory strength, pain relief, and high patient satisfaction.
Wrist motion has been shown to be equal or slightly less than preoperative motion. Grip strength has been reported to range between 64 and 100% of the contralateral normal wrist.4,7,11,12,17–21 In addition, patients may be converted to a wrist arthrodesis or arthroplasty if painful osteoarthritis develops. The disadvantages of proximal row carpectomy include loss of carpal height, an incongruous joint, and possible progression of radiocapitate arthrosis. Imbriglia et al. have shown that the radius of curvature of the capitate is approximately two-thirds of the lunate fossa of the distal radius. Using cineradiography, they demonstrated that the motion of the capitate on the distal radius is translational with a moving center of rotation.21 Imbriglia reported that 12 of 27 patients in his long-term follow-up study developed radiographic evidence of cartilage space narrowing, although without clinical consequence.13
Literature regarding arthroscopic proximal row carpectomy is sparse. There are no long-term studies, although short-term results are promising. The majority of the literature mentions arthroscopy as an available technique for proximal row carpectomy without discussing clinical results.5,22–25
Indications and Contraindications
Proximal row carpectomy26 has also been described in the treatment of failed carpal implants, cerebral palsy, spasticity, acute and chronic fractures and dislocations, and replantation. We do not currently recommend arthroscopic proximal row carpectomy in this latter subset of patients.
Other relative contraindications to proximal row carpectomy in general include degenerative changes of the capitate head or lunate fossa of the distal radius, multicystic carpal disease, and preexisting ulnar translocation of the carpus. Due to the high failure rate of open proximal row carpectomy in patients with inflammatory arthropathy (e.g., rheumatoid arthritis), both Culp et al. and Ferlic et al. do not recommend its use in these patients.4,27
Technique
The patient is positioned supine on the operating table, with the affected arm positioned on a radiolucent hand table. A well-padded arm tourniquet is placed proximal to the arm. The procedure can be carried out under general or regional anesthesia because operative times are generally less than two hours. The wrist is then suspended in a traction tower and 10 to 15 pounds of traction is applied (Figure 26.1). After distraction is obtained, landmarks are outlined on the dorsum of the wrist and the portals are made. The tourniquet is routinely inflated without additional exsanguination. Routinely, the 3-4 portal is the initial viewing portal.

Next, the midcarpal joint must be well visualized to ensure an adequate proximal capitate cartilaginous surface (Figure 26.2). If the status of the capitate joint is questionable, an alternative procedure is performed: four-corner fusion, capitolunate arthrodesis, proximal row carpectomy with interposition arthroplasty, or wrist arthrodesis. Assessment of the midcarpal articular surfaces is accomplished through the radial midcarpal portal, which is approximately 1 cm distal to the 3-4 portal. Arthroscopic instruments that will be needed to perform the proximal row carpectomy include a hook probe, a 2.9 shaver or radiofrequency device, a 4.0 bur, small sharp osteotomes, pituitary rongeurs, and an image intensifier.
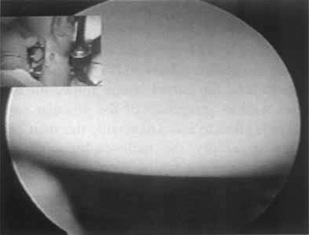
FIGURE 26.2 View from radial midcarpal portal demonstrating a healthy-appearing proximal capitate.
(Reproduced with permission from Culp RW, Osterman AL, Talsania JS. Arthroscopic proximal row carpectomy. Tech Hand and Upp Ext 1997;2(1):116–19).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


