CHAPTER 13 Arthroscopic Dorsal Radiocarpal Ligament Repair
Introduction
In recent years, various investigators have highlighted the role of the dorsal radiocarpal ligament (DRCL) in maintaining carpal stability.1–4 Tears of the DRCL have been linked to the development of both volar and dorsal intercalated segmental instabilities and may be implicated in the development of midcarpal instability.5–7 The existence of a DRCL tear when combined with a scapholunate interosseous ligament (SLIL) tear connotes a greater degree of carpal instability. This has been acknowledged by some authors, who have advocated an open SLIL repair versus arthroscopic pinning when there is an associated DRCL tear.8 An isolated tear of the dorsal radiocarpal ligament can also be a source of chronic wrist pain.9
In most series, the DRCL is overlooked during the typical arthroscopic examination of the wrist. It is difficult to visualize a DRCL tear through the standard dorsal wrist arthroscopy portals because the torn edge of the DRCL tends to float up against the arthroscope while viewed through the 3/-,4 portal and 4/-5 portals, which makes both identification and repair of the DRCL tear cumbersome. It can be seen obliquely through the 1/-,2 or 6-U portals, but visualization of the DRCL across the radiocarpal joint may be laborious in a tight or small wrist—especially if synovitis is present. Wrist arthroscopy through a volar radial portal (VR) is the ideal way to assess the dorsal radiocarpal ligament due to the straight line of sight10–12 (see chapter on arthroscopic portals).
Indications
A classification system for DRCL tears was devised based on the presence or absence of associated carpal pathology (Table 13.1). Each successive stage denotes a longer-standing and/or more severe condition that negatively impacts the prognosis.
Table 13.1 Classification of Dorsal Radiocarpal Ligament Tears
| Stage I | Isolated DRCL tear |
| Stage II | DRCL tear with associated SLIL ± LTIL (Geissler I/II) ± TFCC tear |
| Stage IIIA | DRCL tear with associated SLIL ± LTIL (Geissler III) ± TFCC tear |
| Stage IIIB | DRCL tear with associated SLIL ± LTIL (Geissler IV) ± TFCC tear |
| Stage IV | Chondromalacia with widespread carpal pathology |
The ligament with the highest Geissler grade determines the stage.
DRCL – dorsal radiocarpal ligament
SLIL – scapholunate interosseous ligament
LTIL – lunotriquetral interosseous ligament
TFCC – triangular fibrocartilage complex
An arthroscopic DRCL repair is indicated for stage I, or isolated DRCL tears due to the favorable outcomes that can be achieved.9,13,14 Geissler grade I and II SLIL and/or LTIL ligament injuries are still amenable to arthroscopic treatment. DRCL repairs are also indicated in Geissler grade I and II injuries since repair of a secondary stabilizer may augment the coronal plane stability (Table 13.2). Thermal shrinkage of the ST ligaments can theoretically augment sagittal plane stability of the scapholunate joint. This can be accomplished arthroscopically and is currently under investigation, but no data is available to recommend this procedure as yet. Grade III ligament injuries represent a relative gray area. They can be successfully treated with thermal shrinkage and pinning, which should be augmented with a DRCL repair, but if this is combined with instability of the ulnocarpal joint due to a large TFCC tear and/or Geissler III ligament tear there is a high risk of failure following arthroscopic treatment alone. Grade IV ligament injuries are beyond the realm of arthroscopic treatment and require open repair or reconstruction. Due to the frequent association of DRCL tears when there is a TFCC tear, I would also recommend a DRCL repair if the TFCC tear is treated arthroscopically.
Table 13.2 Algorithm for Treatment of DRCL Tears
| Stage I | Arthroscopic DRCL repair |
| Stage II | Arthroscopic DRCL repair, SLIL or LTIL debridement ± shrinkage, TFCC repair/debridement |
| Stage IIIA | Arthroscopic DRCL repair, SLIL/LTIL shrinkage + pinning, TFCC repair/debridement ± wafer (consider STT shrinkage) |
| Stage IIIB | Open SLIL repair/reconstruction ± capsulodesis, LTIL repair/reconstruction, TFC repair/debridement ± wafer/ulnar shortening |
| Stage IV | Partial carpal fusion vs. PRC |
DRCL – dorsal radiocarpal ligament
SLIL – scapholunate interosseous ligament
LTIL – lunotriquetral interosseous ligament
PRC – proximal row carpectomy
Contraindications
When the treatment of an SLIL tear or dynamic scapholunate instability includes some type of dorsal capsulodesis, the dorsal incision followed by the creation of a dorsal capsular check-rein to restrain palmar flexion of the scaphoid renders any separate treatment of the DRCL tear unfeasible. When the DRCL tear is seen in association with palmar midcarpal instability (MCI), a soft-tissue repair of the dorsal ligaments will not by itself correct the MCI.15,16
Clinical Studies
A retrospective chart review was performed of patients who underwent diagnostic wrist arthroscopy with the use of a volar radial portal.13,14 This identified 53 patients (56 wrists) over a six-year period. Additional pathology was seen in 24 patients that was not visible from the standard dorsal portals. This included 22 patients with tears of the dorsal radiocarpal ligament. Static wrist radiographs were obtained for all patients. Radiographs included a neutral-rotation posteroanterior view and a lateral view. None of the wrists showed a static carpal instability pattern. Magnetic resonance imaging was performed under the direction of the referring physician in six patients. Preoperative arthrograms were performed as a part of the diagnostic work-up for wrist pain in 20 patients.
There were 6 men and 16 women. The average patient age was 40 years (range 25 to 62 years). All patients failed a trial of conservative treatment with wrist immobilization, cortisone injections, and work restrictions. The average length of conservative treatment was seven months. The time interval between injury and surgical intervention averaged 25 months (range 8 to 53 months). At the time of arthroscopy, four patients were found to have an isolated DRCL tear that was solely responsible for their wrist pain. The remaining 17 patients had additional ligamentous pathology, summarized in Table 13.3. A dorsal capsulodesis was performed in seven patients as the primary treatment for derangements of the SLIL.
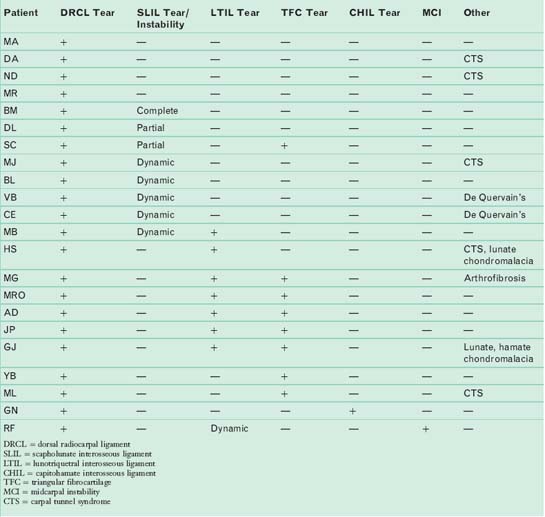
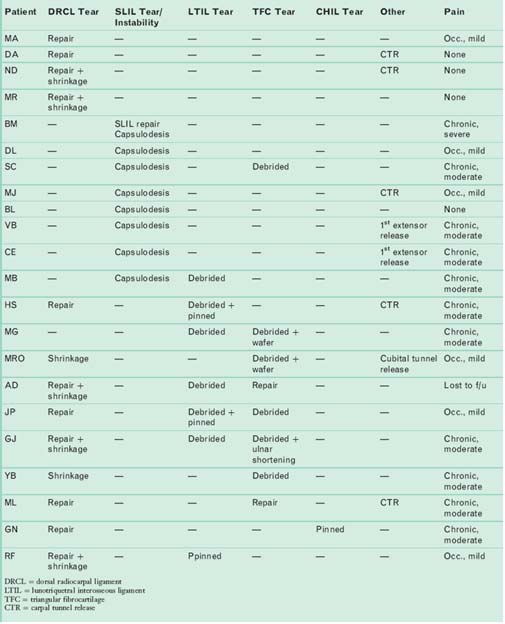
Thirteen of the 21 patients underwent an arthroscopic DRCL ligament repair and/or thermal shrinkage (repair = 5, repair + shrinkage = 6, shrinkage = 2), as described in material following. Ten of these patients underwent ancillary procedures for treatment of the coexisting wrist pathology. Lunotriquetral tears were treated with debridement and pinning. Triangular fibrocartilage tears were debrided or repaired. Scapholunate ligament tears or instability was treated with capsulodesis ± repair. One patient had generalized arthrofibrosis (MG), which precluded a DRCL repair. Concomitant nerve entrapment was a common finding, which was treated at the same time.
The average duration of the follow-up period was 16 months (range 7 to 41 months), with one patient lost to follow-up at four weeks. Pain was graded as none, mild, moderate, and severe.17 Wrist extension, wrist flexion, radial deviation, ulnar deviation, and grip strength were assessed. Wrist range of motion was compared with presurgical values. Grip strength was compared with the contralateral side at follow-up evaluation.
Patient outcomes are summarized in Table 13.4. The four patients who underwent an isolated DRCL repair were satisfied with the outcome of surgery and would repeat the surgery again because it improved their symptoms. All four patients graded their pain as none or mild. None of these patients were taking pain medications. All returned to their previous occupations without restriction. Their wrist motion was unchanged compared to the preoperative status. Grip strengths were 90 to 130% of the opposite side. The wide variety of ancillary procedures in the remaining patients and the small numbers in each subgroup precluded any statistical analysis of the possible influence of the DRCL repair on wrist motion and grip strengths.
< div class='tao-gold-member'>
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


