Double Arthrodesis Through a Medial Approach for End-Stage Adult-Acquired Flatfoot
Alan R. Catanzariti, DPM∗acatanzariti@faiwp.com and Adebola T. Adeleke, DPM, Division of Foot & Ankle Surgery, West Penn Hospital, 4800 Friendship Avenue, N1, Pittsburgh, PA 15224, USA
∗Corresponding author. 4955 Steubenville Pike, Suite 189, Pittsburgh, PA 15205.
Triple arthrodesis has traditionally been the procedure of choice for end-stage adult-acquired flatfoot. The results have been universally good, and it has proven to be dependable and predictable. Nonetheless, complications have been reported following triple arthrodesis in certain patients. Selective arthrodesis of the talonavicular joint and subtalar joint through a single medial approach has been developed as an alternative. The authors especially prefer this procedure with severe transverse plane deformity and often choose this approach as an alternative to triple arthrodesis in high-risk patients, including those patients with diabetes mellitus, rheumatoid arthritis, long-term steroid use, and the elderly.
Introduction
Triple arthrodesis has traditionally been the procedure of choice for end-stage adult-acquired flatfoot. The results have been universally good, with relatively high patient satisfaction. Furthermore, triple arthrodesis has proven to be a dependable and predictable procedure. Nonetheless, complications have been reported following triple arthrodesis in certain groups of patients. These complications include an increased risk of degeneration in surrounding joints, inadequate realignment when severe transverse plane deformity exists, increased risk of a residual supinatus/varus deformity in patients with severe peritalar subluxation, and lateral wound problems in patients with a combination of severe valgus deformity and deficient lateral skin.1–6 Additionally, the calcaneocuboid joint (CCJ) may require bone grafting following realignment of a severe deformity.7
Selective arthrodesis of the talonavicular joint (TNJ) and subtalar joint (STJ) through a single medial approach has been developed as an alternative surgical option to help avoid or diminish the incidence of complications sometimes encountered with triple arthrodesis.8–16 Indications for this procedure include end-stage adult-acquired flatfoot (stage III or IV) when deformity is usually severe and nonreducible. The authors especially prefer this procedure with severe transverse plane deformity, where an Anteroposterior (AP) radiograph demonstrates severe subluxation or dislocation of the TNJ. This procedure is also ideal in those patients with a combination of severe deformity and deficient lateral skin that might predispose them to lateral wound dehiscence following realignment. The authors often choose this approach as an alternative to triple arthrodesis in high-risk patients, including those patients with diabetes mellitus, rheumatoid arthritis, long-term steroid use, and the elderly.
Technique
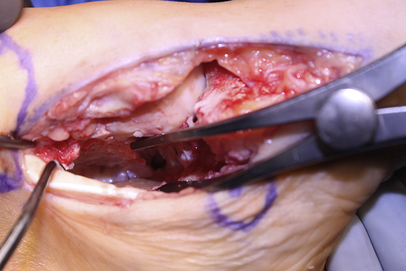
The procedure is performed through medial incision beginning just posterior to the medial malleolus and extending to the medial cuneiform. The authors sometimes carry the incision further distally if a naviculocuneiform or first tarsometatarsal arthrodesis is part of the reconstruction. A full-thickness incision is made just dorsal to the posterior tibial tendon. The tendon is inspected, and if severe tendinosis is noted, the entire tendon is evacuated. If, however, the tendon appears to be viable and healthy, the tendon is preserved. A complete release of all periarticular structures about the TNJ and STJ, including the interosseous and bifurcate ligaments, is essential. This permits adequate intra-articular visualization for cartilage debridement and joint preparation. Additionally, thorough release of contracted soft tissue structures allows easier reduction of the deformity. However, caution should be exercised during proximal dissection about the malleolus with care taken to avoid excess transection of the anterior portion of the deltoid ligament. Overzealous transaction of the anterior portion of deltoid ligament might predispose the ankle to valgus deformity, especially if hindfoot realignment is not adequate. Furthermore, the authors typically identify the flexor hallucis longus tendon, and sometimes, the flexor digitorum longus tendon, and protect them throughout the case. A combination of lamina spreaders and pin distractors can then be utilized to provide access to the STJ. Sharp, curved osteotomes and currettes are used to debride the cartilage. Angled Currettes are ideal for debriding cartilage from the posterior facet. After the distractors have been present for a period of time, and the cartilage has been debrided from the posterior facet, the posterior-lateral joint capsule is visible (Fig. 1). The authors carefully release this structure. All debris is then evacuated from the STJ prior to joint preparation. This includes soft tissue structures distal to the articular surfaces, as the authors will prepare this area for arthrodesis to extend the fusion mass into the extra-articular area. The TNJ is then distracted for cartilage debridement and joint preparation in the same manner. Following lavage of both joints, the subchondral plates are fenestrated and weakened with a 2.5 mm drill and then methodically broken with a small osteotome (Fig. 2). The authors often augment these sites with demineralized bone matrix gel. The STJ is reduced into a neutral position, and the TNJ is then realigned and provisionally fixated with guide pins from a 4.5 mm cannulated screw system. This maneuver is performed under image intensification, checking AP, lateral, and axial images. The authors typically deliver the first screw medially, from the navicular tuberosity, to support realignment. The second screw is delivered percutaneously along the most lateral aspect of the TNJ. A third screw is sometimes delivered centrally. It is important to have even compression across the entire TNJ. The STJ is then fixated with 2 large-diameter cannulated screws delivered from inferior to superior (Fig. 3). The authors then perform a valgus stress test of the ankle under image intensification and proceed to repair the deltoid ligament if valgus is found. The wound is then closed in standard fashion over a closed suction drain. Patients are placed into a nonweight-bearing short-leg cast for 6 to 8 weeks, followed by a fracture boot for an additional 3 to 4 weeks. Postoperative decisions are based on serial radiographs and clinical findings such as edema and warmth.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


