Chapter 3 Aquatic Physiotherapy
Treatment methods
• The physical properties of water covered in the assessment chapter facilitate the application of treatment techniques that can be used to provide therapeutic benefits for patients managed in a pool. Methods of utilising these physical properties of water are as follows.
Uses of buoyancy
The grading of muscle actions in water
• Muscle strength is graded on land according to the Oxford or Muscle Test Rating scales. In water these scales are modified so that muscle strength can be finely graded utilising hydrodynamic principles. As on land this scale is subjective, especially when there is no ‘normal’ limb to compare against.
Muscle strength grading in water
Grade 2− Buoyancy counterbalanced
Grade 2 Buoyancy counterbalanced with speed
Grade 3 Against buoyancy with small float or with speed
Grade 3+ Against buoyancy with larger float
Grade 4 Against buoyancy unstreamlined
Grade 4+ Against buoyancy with large float with speed
Grade 5 Against buoyancy unstreamlined with maximum speed or with largest float able to be moved
Muscle actions during immersion
Concentric
Buoyancy assisted Moving a limb or body part towards the water surface
Buoyancy counterbalanced Any movement of a limb or body parallel to the water surface
Buoyancy resisted Movement of a limb or body part downwards against the upward thrust. This resistance can be increased by the use of additional flotation aids, or by lengthening the lever arm.
Isometric
This type of muscle action can be achieved by:
• Buoyancy Maintaining the position of a limb or body part against the upthrust forces.
• Metacentre Holding an adopted position with altered body shape against the rotational forces caused by an imbalance between the forces of buoyancy and gravity.
• Turbulence Holding the position of a limb or body part against the drag created by an area of turbulence (low pressure water) created by the physiotherapist.
• Drag effect Holding a posture against the drag effect created when the therapist moves a patient through the water.
The latter two effects can equally be used to promote concentric dynamic muscle action.
Muscle strengthening: using buoyancy, turbulence and the metacentric effect
Buoyancy
Resisted concentric
• The body part is moved away from the water surface – limbs will need a flotation aid due to their higher relative density, e.g. to strengthen the left shoulder adductors a float is held in the left hand. The patient stands, leaning over to their left side with the shoulder immersed. The left arm is pulled down from the surface through the water to come to the patient’s side.
• These techniques are generally written as ‘buoyancy resisted’.
Resisted eccentric
• The patient has a hand float attached around an ankle and the ankle is allowed to be taken towards the surface, passively flexing the knee. The patient controls the rate of movement of the ankle, so that it rises to the surface at a slower rate than the float is trying to take it. For example, an eccentric quadriceps exercise requires the patient to stand at the pool side with a float round their ankle. They let the knee flex slowly so that the float gradually moves towards the surface.
• These techniques are generally written as ‘buoyancy resisted’.
Utilising turbulence
Therapist created
• The therapist creates an area of fast-moving water to create drag on a body part. The patient resists movement towards this area of low pressure, e.g. to create resistance for the biceps. The patients arm is supported on a float at water surface. The therapist then creates turbulence over the posterior forearm and outwards.
• These techniques are generally written as ‘turbulence resisted’.
Patient created
• The patient moves a body part through the water, thus creating an area of low pressure behind the moving part, e.g. to create a strengthening exercise for the shoulder flexors and extensors the patient moves their arm briskly backwards and forwards through the water.
• These techniques are generally written as ‘speed resisted’.
Via the ‘drag’ effect
• The patient is moved through the water while they hold a position against the drag of the water. For example, to strengthen the trunk side flexors the patient is supported supine on floats. The therapist holds the patient either at the ankles or the shoulders and swings them sideways through the water while the patient tries to prevent side flexion.
• These techniques are generally written as ‘drag resisted’.
Utilising the metacentric effect
• The patient holds a position against the turning forces created, e.g. patient in supine lying, works against the following movements to prevent the tendency for the body to rotate along its longitudinal axis:
• Patient in standing or in the ‘box position’ (squatting in the water as if sitting on a chair), supine lying, works against the following movements to prevent the tendency for the body to rotate around its transverse axis:
• These techniques are generally written as ‘metacentre resisted’.
Physiological considerations
• Comparing oxygen consumption and heart rate responses during exercises performed on land and in the water, both heart rate and oxygen uptake are greater during exercises in water.
• Evidence indicates that viscosity and turbulence provide a greater load during exercise than the resistance of gravity during land exercises.
• Oxygen consumption increases by about ten times over resting values in the water for male subjects performing leg exercises and about seven times for women.
• Arm exercises performed in water require less energy than leg exercises in water.
• However arm exercises require significantly more oxygen when performed in water than the same exercises performed on land (Johnson et al 1977).
Improving range of movement (ROM)
Utilising buoyancy
Buoyancy assisted
• The body part is moved towards the water surface, assisted by a float. This can be done as a contract/relax technique or as a prolonged stretch (Figures 3.1–3.17).
• These techniques are generally written as ‘buoyancy assisted’.
• Therapist created turbulence can be added to assist the effect.











The lower limb stretches
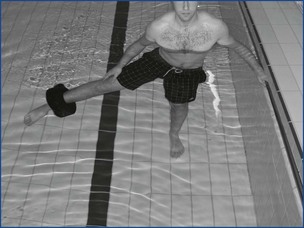
• Keep trunk upright allow float to take leg up towards surface of pool (Figure 3.1).
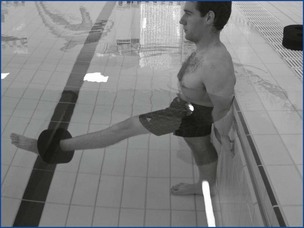
• Trunk braced against poolside, patient instructed to hold a lordosis, allow float to take leg up towards surface of the pool (Figure 3.2).
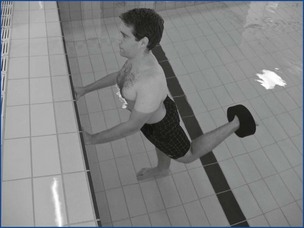
• Patient holding onto side of pool (elbows flexed to help keep body upright). Patient flexes left knee and hip to eliminate lumbar hyperextension (Figure 3.3). Allow float to take leg towards surface of pool, patient instructed to keep knee in extension.
• Patient holding side of pool with elbows extended. With left hip and knee flexed, allow float to bring the flexed leg towards pool surface (Figure 3.4).
• Patient with trunk braced against pool side, right hip flexed to 90°, right hand to fix knee to enable rotation around axis of femur to occur. Allow float to bring the foot up (Figure 3.5).
• As per stretch for lateral rotators, but with opposite rotation of femur (Figure 3.6).
• Patient holds side of pool to keep trunk upright and thigh in neutral position. Allow float to bring foot up towards pool surface (Figure 3.7).
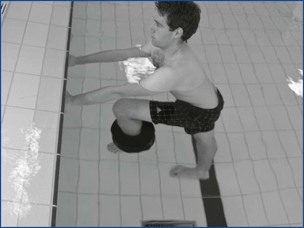
• Patient facing pool side with both forearms on rail. Tread on inside of inner surface of ring. Twist knees to R and flex both up the wall to the R so that L thigh is against wall. Both feet and float remain under the knees (Figure 3.8).
• Patient in standing or sitting on stool, flex hip to 90°. Patient to fix thigh position and allow float to bring foot up to surface of pool (Figure 3.9).
• Patient with trunk horizontal to water surface, left hip in 90° flexion, allow float to take foot up to surface of pool (Figure 3.10).
The upper limb stretches
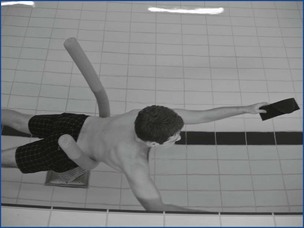
• Patient supported by floats in right side lying, facing side of pool. Keeping elbow extended allow wrist float to bring the arm through abduction to surface of pool (Figure 3.11).
• Patient with trunk parallel to pool surface with waist float. Keep elbow in extension allow float to bring hand to surface of pool (Figure 3.12).
Trunk stretches
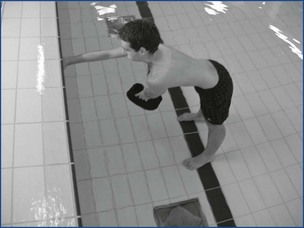
• Patient prone, keeping knees extended allow float to bring legs to surface of pool, producing spine extension (Figure 3.13).
• Patient to grasp side of pool, keeping shoulders level and thighs against pool side, allow float to bring the legs up towards pool surface (Figure 3.14).
• Patient holding pool side with feet fixed on pool floor. Allow float under scapulae to bring trunk up to pool surface (Figure 3.15).
• Patient grasps pool side with right arm in extension. Patient reaches under the trunk with left arm and allows float to take the hand up to pool surface (Figure 3.16).
• Patient with float under hips and float around ankles allowing feet to float to surface of pool, keeping thighs in the water (Figure 3.17).
• The stretches can also be carried out as slow prolonged stretches, using flotation and the same starting position as described in Figures 3.1–3.17. With this type of stretch the end position with buoyancy providing the stretch should be maintained for 30–60 seconds.
Stretches using drag
• Some muscle groups can also be stretched using the principles of drag. In most instances the patient needs to be supported on floats and the body moved through the water in a direction which provides drag on the muscle group to be stretched, e.g. the patient lies supine supported by floats, while the therapist grasps either the shoulders or lower legs and moves the patient in an arc to the right, which will stretch the right side flexors.
• Stretch can be increased by increasing the speed of movement and/or by increasing the length of the moving lever.
• For these stretches to be effective the patient must be able to relax whilst lying on floats.
Specific stretches using drag
| Muscle group | Starting position |
|---|---|
| Trunk side flexors | Supine lie |
| Trunk rotators | Supine lie, therapist adds rotation as the body moves through an arc |
| Trunk flexors/extensors | Side lie |
| Hip adductors | Supine lie |
| Shoulder adductors | Supine lie |
| Shoulder extensors | Prone or side lie |
| Pectorals | Standing – walking forwards holding bats in both hands |
| – walking in a circle holding a bat in the hand of the arm to be stretched | |
| Elbow flexors | Standing – walking forwards holding bats in both hands |
| – walking in a circle holding a bat in the hand of the arm to be stretched |
Therapeutic methods developed to utilise the properties of water
The Bad Ragaz Ring Method (BRRM)
Bad Ragaz, background
• In the 1930s, land exercises were applied in water without attention to the properties of water, Dr Knupfer from Germany developed exercises where the physiotherapist acts as a fixed point for movement and the patient is supported in supine lying with pelvic and neck floats.
• During the 1940s and 1950s the polio epidemic in the USA led to the development of the proprioceptive neuromuscular facilitation (PNF) techniques by Knott and Voss in the USA during the 1960s (Voss et al 1985).
• Bad Ragaz techniques were developed through a combination of the earlier German techniques and the PNF techniques in Bad Ragaz, Switzerland, which gives the method its name.
• The most significant developments of the Bad Ragaz Ring Method (BRRM) took place between the early 1960s and 1990. Initially these techniques were developed by Dr Zinn and Nele Ipsen and later by Bridget Davies and Beatrice Egger who published articles outlining the therapeutic processes and the benefits to be gained from this form of therapy (Davies 1967, Zinn 1975, Egger and Zinn 1990).
Features of BRRM
• The method utilises the properties of water of turbulence and streamlining, with buoyancy being used as a support and not as a means of resistance during exercise.
• Turbulence provides resistance due partly to negative pressure behind the moving body i.e. ‘negative drag,’ resulting from the formation of eddy currents, which impede forward movement.
• Turbulent drag is directly proportional to the speed of movement through water, therefore the faster the patient moves, the greater the resistance. This is controlled by the patient and therefore the method is ‘self regulating’.
• It restores anatomical, biomechanical, physiological movements of joints and muscles in functional patterns.



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


