Anterior Spinal Column Reconstruction: Anterior, Lateral, and Oblique Approaches to the Spine
Anterior Lumbar Interbody Fusion
Introduction
Lumbar levels from L2 to sacrum can be accessed via a single retroperitoneal approach
Patient Selection
Indications
Anterior lumbar approach most often performed at L4-L5, L5-S1, with single-level fusion through retroperitoneal approach most commonly
Most common indication for single-level lower lumbar spine surgery is lumbar disk degeneration with low back pain
Others include diskitis/osteomyelitis, nonunion after posterior fusion procedure, spinal deformity surgery, recurrent disk herniation, total disk replacement/revision, fractures, tumor surgery
Failure of nonsurgical treatment
Alternatives include transabdominal or laparoscopic approaches; both associated with more complications, including prolonged postoperative ileus, bowel injury, retrograde ejaculation
Contraindications
Revision setting, particularly L4-L5; L5-S1 may be approached from side opposite index approach without significantly increasing vascular injury risk
Direct lateral approach to levels above L5-S1 may be safer than revision anterior surgery
Diagnosis
Diagnosis of degenerative disk disease most commonly encountered at L4-L5, L5-S1; may see multilevel disease
Presents with long history of low back pain with exacerbations over many years
Preoperative Imaging

Figure 1Lateral radiograph shows a loss of disk space height at L5-S1.

Figure 2Sagittal T2-weighted MRI demonstrates typical changes associated with a symptomatic lumbar degenerative disk.
Plain radiographs demonstrate height loss on lateral view (Figure 1)
Instability on flexion-extension imaging uncommonly may coexist with degenerative disk
Be aware of spondylolysis affecting involved motion segment; may affect need for additional fixation
May see vacuum disk sign on standing, recumbent, flexion-extension radiographs
MRI changes may include loss of disk space height, loss of signal intensity in nucleus pulposus on T2-weighted image, posterior disk bulge on axial imaging, Modic end-plate changes (Figure 2); may see compression of neural elements on axial imaging affecting central canal, subarticular recess, or far lateral zone of neural foramen
Procedure
Room Setup/Patient Positioning
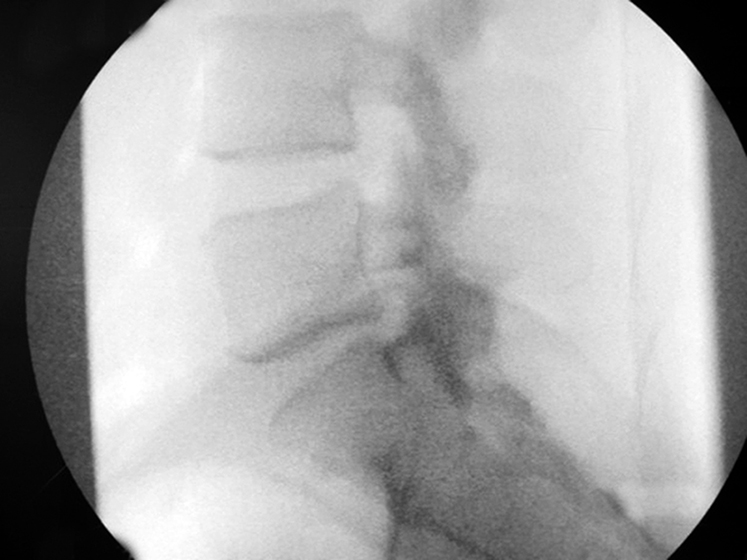
Figure 3True lateral fluoroscopic image demonstrates disk collapse at L5-S1.

Figure 4Photograph depicts a flat Jackson OSI table. The patient’s arms are folded over the chest to allow intraoperative fluoroscopy in the lateral plane.

Figure 5A Mizuho OSI Jackson Axis table in the flat position.
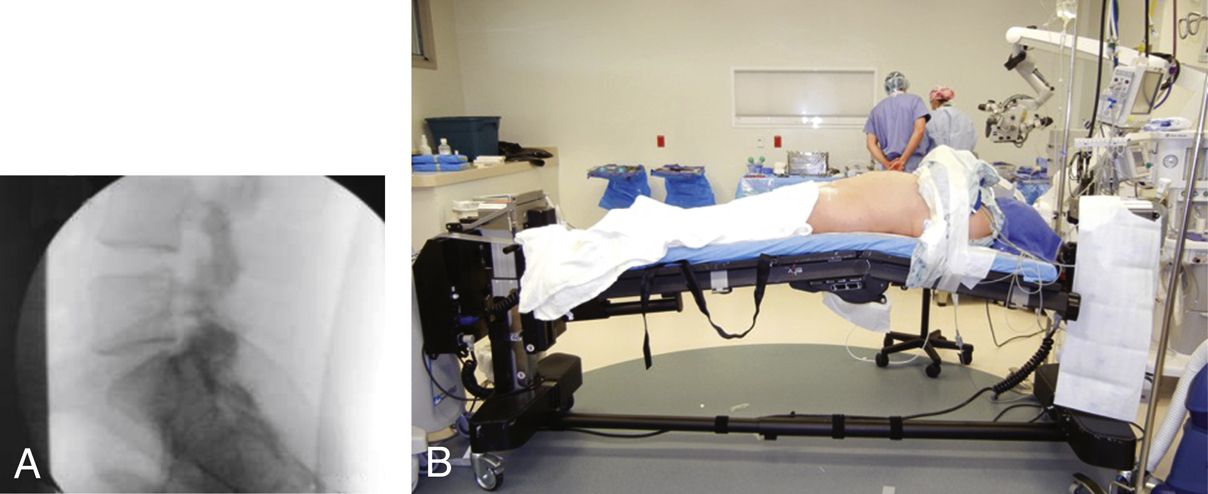
Figure 6Note the increased lordosis at L5-S1 as seen on a lateral fluoroscopic image (A) with extension of the operating table using the extension function of the Axis table (B).
Use operating table that allows intraoperative fluoroscopic imaging (Figure 3)
Author prefers flat Jackson OSI table (Figure 4) or Jackson Axis OSI table (Figure 5) (Mizuho OSI); Axis table allows flexion or extension, creating more or less lumbar lordosis (Figure 6); may benefit deformity cases or collapsed disk space
Alternatively, can place inflatable arterial line cuff under lower lumbar spine as bolster to increase lumbar lordosis
Position patient on operating room table with care to ensure no rotation of pelvis or torso; pad appropriately
Special Instruments
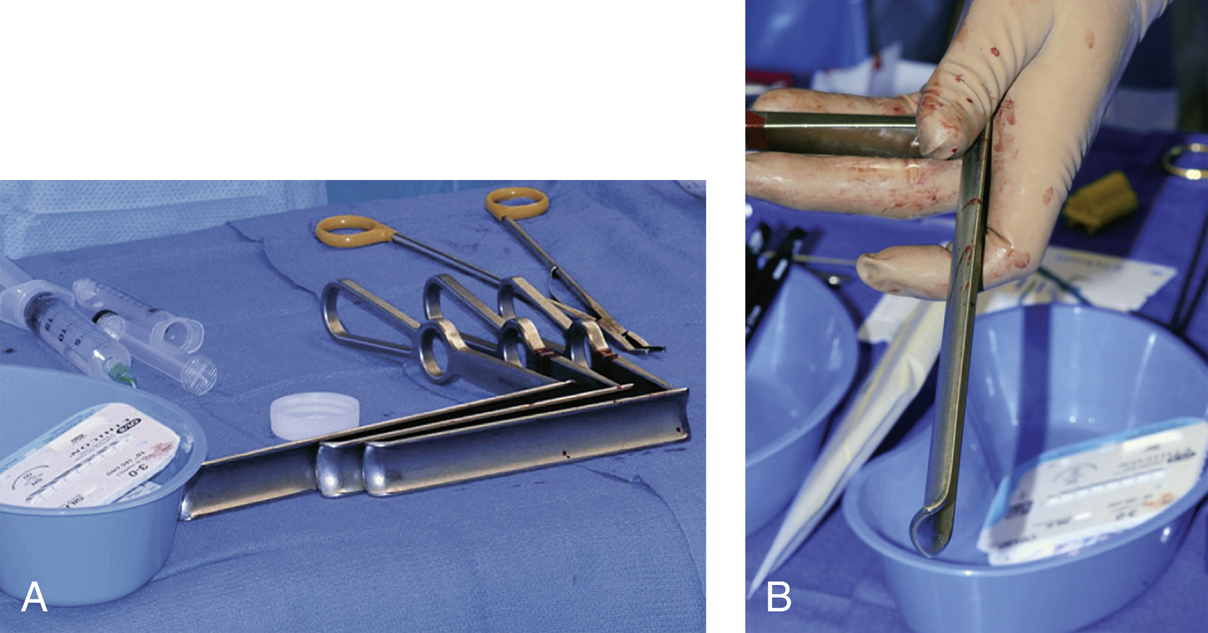
Figure 7Photographs of the instruments used for anterior lumbar interbody fusion. A, Handheld vascular retractors of various lengths. B, Note the gentle curve at the tip of the vein retractor to assist with retraction and visualization.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


