31
ANTERIOR (SMITH–PETERSON) APPROACH
USES
This approach is used for hip flexor lengthenings or releases, for access to the psoas tendon and the psoas bursa underneath that tendon, and for draining infections of the hip in children. Campbell calls the Smith-Peterson approach an anterolateral approach. Rockwood and Green list it as an anterior approach and call it the iliofemoral approach to the pelvis. The description here is an expanded version of the distal portion of their iliofemoral approach.
ADVANTAGES
This approach comes through the internervous plane between the sartorius and the tensor fascia lata. It also uses the pectineus to protect the femoral neurovascular structures. It does not interfere with blood supply to the hip capsule, which is very important in children.
DISADVANTAGES
This approach provides limited lateral exposure and no posterior exposure to the hip.
STRUCTURES AT RISK
Probably the most commonly injured structure with this approach is the lateral femoral cutaneous nerve, which usually exits the pelvis close to the anterosuperior iliac spine and runs in an oblique course down the thigh. The nerve is typically found in the lateral flap of this approach, but if it crosses more medially than is normal, it may need to be sacrificed and allowed to retract into the pelvis.
The other structures at risk are the femoral nerve and artery. The nerve sits more laterally than the artery and is encountered first. Additionally, it gives off branches to the sartorius, and if there is any dissection along the medial aspect of the sartorius, that muscle can be denervated. This nerve is anterior to the pectineus muscle, which is generally used to protect the nerve. It may branch fairly high, sending off its motor branches to the sartorius and the rectus.
The approach usually requires the release of the rectus femoris to obtain adequate hip exposure. If that is not approximated well, then that muscle function can be compromised.
When you are deep to the rectus femoris muscle and have the iliacus and psoas tendon in view, the medial femoral circumflex artery can be damaged. It generally is approximately 1 cm proximal to the lesser trochanter and is closely approximated to the tendon. The artery is large and will bleed profusely if not protected.
TECHNIQUE
An incision starts generally below the anterosuperior iliac spine, running distally, generally paralleling the sartorius muscle. It is carried through subcutaneous tissue. If the lateral femoral cutaneous nerve is identified, it is usually retracted in a medial direction. The first muscle encountered is the sartorius muscle, which is identified by the direction of its fibers from the anterosuperior iliac spine running in a medial direction. Lateral to it are the tensor fascia lata muscles, whose fibers are originating in the same location and along the iliac crest going posteriorly. As you move distally, the interval between these two muscles is easily developed. Deep to those muscles is the rectus femoris, which is in its own sheath, going up to the anteroinferior iliac spine; it usually needs to be released. When this is done, the anterior capsule is identifiable. Deep to the rectus, again in their own sheaths, are the iliacus and psoas tendons, which generally do not need to be disturbed in the approach to the hip itself.
TRICKS
The key trick is identifying the interval between the sartorius and the tensor fascia. As long as you stay lateral and deep to the sartorius, the femoral nerve and artery will be protected.
HOW TO TELL IF YOU ARE LOST
It is difficult to get lost in a lateral direction because you will simply run into the subcutaneous tissue lateral to the tensor fascia. It is quite possible, however, to get lost medially and put the femoral nerve at great risk. The key is the sartorius muscle, whose fibers are long and coming off of the iliac spine. It is a discrete muscle in its own fascial sheath that is easy to identify. If you do not see those fibers running from the anterior spine in a distal medial direction, but are seeing fibers only running longitudinally along the leg, then something is wrong. Once you are deep to the sartorius, you will see the longitudinal fibers of the rectus. The rectus muscle is in a discrete sheath, whose medial border protects the psoas tendon. You should see the longitudinal fibers of the rectus and the discrete sheath. If you are deep to the sartorius and you do not see them you are probably too far lateral. If you see fibers coming directly off of the proximal femur, you are looking at the origin of the vastus intermedius and are too far distal. If you see fibers running from the midline of the body toward the femur, you are looking at the pectineus muscle. Be careful, because the nerve, artery, and vein are just anterior to the pectineus.
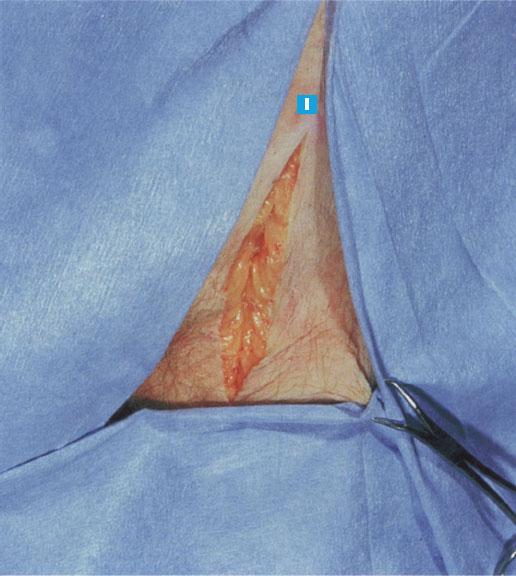
FIGURE 31–1
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


