23
Anterior Shoulder Instability: Arthroscopic Suture Anchor Repair of the Bankart Lesion
The open Bankart repair is the “gold standard” for treating recurrent anterior instability of the shoulder. Repair of the capsulolabral complex can be performed arthroscopically to duplicate the open technique, using suture anchors. Prior arthroscopic procedures for correcting anterior instability have had a higher failure rate than open procedures, but with the use of suture anchors, the results have improved and are now approaching the results of the open technique.
Indications
Recurrent anterior instability from a traumatic etiology that produces an avulsion of the anterior labroligamentous complex.
Contraindications
1. Large Hill Sachs lesion
2. Large bony Bankart lesion
3. Poor-quality ligament or labral tissues
Relative Contraindications
1. Multidirectional laxity with a Bankart lesion
2. Contact sports
3. Revision surgeries
Mechanism of Injury
The shoulder is placed in a position of abduction, external rotation, and extension, tearing the labrum and ligaments from the anterior rim of the glenoid.
Physical Examination
1. Apprehension in the abducted, externally rotated, and extended position
2. Increased translations of the involved shoulder
Diagnostic Tests
1. Standard anteroposterior and axillary lateral X-ray shoulder views.
2. WestPoint axillary lateral if there is suspicion of a bony Bankart lesion.
3. Internal rotation Hill Sachs views if there is suspicion of a large Hill Sachs lesion.
4. A computed axial tomography scan may be indicated in the multiply dislocated shoulder with significant bony changes on the glenoid or humerus.
Preoperative Planning and Timing of Surgery
The repair of first-time anterior shoulder dislocations is controversial. This is probably only necessary in the rare individual who is a high-level athlete. However, arthroscopic repairs are easier and have a better outcome if they are performed early in the course of the patient’s instability. For example, operating after only two or three episodes of instability rather than 10 or 20 episodes offers a better outcome.
Special Instruments
1. Complete arthroscopic setup including shaver system and shoulder traction device
2. Fastak 2.8 mm metal suture anchor (Arthrex)
3. Special drill guide and Spear (Arthrex)
4. Suture lasso (Arthrex)
5. 7 mm clear cannula (Arthrex)
6. Crochet hook (Linvatec)
7. Crab claw (Arthrex; Linvatec)
Anesthetic Options
1. General anesthesia is preferred.
2. Scalene block can be used.
Patient and Equipment Position
1. Lateral decubitus position (Fig. 23–1).
2. Shoulder holder on the posterior side of the patient to allow for adequate forward flexion of the arm.
3. The arm is prepped and draped free, and wrapped in a sterile arm sleeve connected to 10 to 15 lbs of traction.
4. Ideal position of the arm is forward flexion of approximately 20 to 30 degrees and abduction of only 30 degrees. This relaxes the anterior capsular structures, giving better exposure for the anterior repair.
Surgical Approach
1. A standard posterior arthroscopic portal is established and a diagnostic arthroscopy is performed, confirming the Bankart lesion.
2. An anterior-superior portal is established from the outside in, just medial to the anterolateral corner of the acromion. A spinal needle is placed in this position to confirm adequate position, and a cannula is inserted (Fig. 23–2A).
3. The standard anterior portal is then established just above the subscapularis tendon. Again, this is made from the outside in, to avoid crowding of the anterior portals; this is positioned just lateral to the tip of the coracoid. A spinal needle is used to confirm proper position. It is important that this portal is lateral (and not too medial), to allow a proper angle for insertion of a suture anchor on the anterior glenoid rim. A lateral position allows the drill guide to be positioned on the anterior rim at a 45-degree angle to the articular surface. A 7 mm clear cannula is inserted.
4. Using the anterior-superior and anterior portals, the anterior glenoid rim is prepared by removing fibrous tissue from the rim down to a bony bed. Use an elevator to mobilize the capsuloligamentous structures. Shavers are used to remove the tissue between the glenoid and the labrum with very minimal burring. Adequate mobilization of the Bank-art lesion must be accomplished to the 6 o’clock position. “Turning the corner” at the 5 to 6 o’clock position is very important to allow adequate repositioning of the labrum back on top of the glenoid. With adequate mobilization, the subscapularis muscle is seen underneath the labroligamentous complex. This is a very important step. If the ligamentous-labral tissues cannot be mobilized and brought back to their anatomic position on top of the articular cartilage anteriorly, then the arthroscopic procedure should be abandoned and an open technique used. Always check with a grasper to assure adequate reduction of the ligamentous-labral tissues before proceeding any further.
5. At this point, a drill guide is inserted through the anterior portal to see if the suture anchor can be placed at the 5 o’clock position through this portal. If this cannot be accomplished, an accessory anterior inferior portal is created. This is accomplished by placing a spinal needle parallel to the cannula that is in the anterior portal, from the outside in. This portal is lateral to the coracoid and 1 cm below it. Anatomic studies have shown the safety of this portal. This portal is only 1 cm lower than the standard anterior portal. When a spinal needle is positioned showing adequate placement into the glenohumeral joint through the subscapularis tendon, a mini-portal is created in that position. This portal is used without a cannula and only needs to be large enough to accommodate the Arthrex Spear and drill guide (approximately 3 mm) (Fig. 23–2B).
6. The blunt spear is first placed through the drill guide tenting the subscapularis, which can be seen arthroscopically. A blunt spear must be used first because the cephalic vein is in close proximity with this inferior portal. (No incidents of bleeding or cephalic vein injury have been documented using this approach.)
7. Once the tenting of the subscapularis tendon is seen, the blunt spear is switched to the sharp spear and pushed into the glenohumeral joint. It is necessary to switch to the sharp trochar because the subscapularis tendon is too thick and strong to be penetrated using a blunt instrument. Once this is inserted, the sharp trocar is removed and the drill guide positioned on the anterior rim at the 5 o’clock position.
8. The arthroscope is then placed in the anterior-superior portal for inserting the suture anchors and sewing the anterior ligamentous-labral complex. With the arthroscope in the anterior-superior portal, orientation is sometimes difficult because the biceps cannot be seen, as it is behind and adjacent to the arthroscope. To help with orientation, before the arthroscope is moved to the anterior-superior portal, notch the glenoid rim at the 3 o’clock or 6 o’clock position with a small burr.
9. A 2.8 mm suture anchor is then drilled into the anterior rim at the 5 o’clock position. The ideal position is just on the edge of the articular cartilage at an angle of 45 degrees to the glenoid in a lateral-to-medial direction. Placing a switching stick through the posterior portal parallel to the glenoid will help with this medial/lateral orientation. A 2.8 mm Fastak anchor is a one-step anchor that is screwed into the bone with power and does not require predrilling. It is best used with a slow-speed drill. This anchor has a #2 Ethibond permanent suture attached through its eyelet. There are marks on the insertion guide to help determine the proper depth of insertion for the anchor. Insertion of the anchor too deeply prevents the suture from sliding in the eyelet. If the anchor is prominent, this can lead to articular damage on the humeral head (Fig. 23–3).
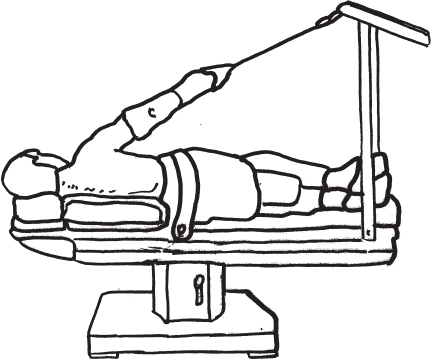
Figure 23–1 Outside view of a patient in the lateral decubitus position with the arm in traction. The arthroscope is in the posterior portal.
Related posts:
 DISTAL CLAVICLE FRACTURE DISLOCATIONS
DISTAL CLAVICLE FRACTURE DISLOCATIONS
 ARTHROSCOPIC SUBACROMIAL DECOMPRESSION: POSTERIOR (CUTTING BLOCK) APPROACH
ARTHROSCOPIC SUBACROMIAL DECOMPRESSION: POSTERIOR (CUTTING BLOCK) APPROACH
 ANTERIOR SHOULDER INSTABILITY: ARTHROSCOPIC SUTURE CAPSULORRAPHY
ANTERIOR SHOULDER INSTABILITY: ARTHROSCOPIC SUTURE CAPSULORRAPHY
 ADHESIVE CAPSULITIS: OPEN CAPSULAR RELEASE
ADHESIVE CAPSULITIS: OPEN CAPSULAR RELEASE
 RECURRENT POSTEROLATERAL ROTATORY INSTABILITY OF THE ELBOW
RECURRENT POSTEROLATERAL ROTATORY INSTABILITY OF THE ELBOW
 EMDIAL EPICONDYLE SURGERY
EMDIAL EPICONDYLE SURGERY
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


