Anterior Cruciate Ligament Injury Prevention: Concepts, Strategies, and Outcomes
Allston J. Stubbs
Mininder S. Kocher
Introduction and History
A recent 10-year survey of knee injuries in 6,434 patients revealed that tears of the anterior cruciate ligament (ACL) were responsible for 20% of joint complaints.1 It is estimated that each year between 75,000 and 250,000 individuals in the United States will suffer a new injury to the ACL. The burden of disease is particularly high in the female athlete. It is estimated that 1.4 million women and girls have torn their ACL during the last decade, and the incidence of noncontact ACL injury in female collegiate athletes is as high as 1 in 10.2
The epidemic of ACL injuries in both noncontact and contact athletics has resulted in a two-pronged strategy of prevention and treatment. As surgical treatment for ACL injuries carries with it morbidity, long rehabilitation and recovery, and large costs, attention has been focused on prevention of the sentinel ligament injury. During the last 35 years, orthopaedic research has contributed to a better understanding of cruciate ligament biomechanics, physiology, and failure patterns. ACL injury prevention models have been developed to address differences in cruciate injury among female athletes3 4 5 6 and contact athletes.7 8 9
A complete tear of the ACL has been historically regarded as a significant injury. This opinion was based on the morbidity of surgical treatment, the length of time for recovery and rehabilitation, and the cost of medical treatment. The evolution of arthroscopic knee surgery, with reliable ligament reconstruction techniques, has limited the associated surgical morbidity of ACL treatment, but issues of recovery time and cost remain. Typically, ACL reconstruction requires a minimum of 6 months of functional therapy to ensure adequate muscle strength and knee joint proprioception. Additionally,
the direct medical costs of a torn ACL approach $17,000 within the first year; a cumulative yearly cost of $1.5 billion in the United States.4 This figure does not account for long-term cost of posttraumatic knee osteoarthritis or emotional cost of a major injury to active individuals.
the direct medical costs of a torn ACL approach $17,000 within the first year; a cumulative yearly cost of $1.5 billion in the United States.4 This figure does not account for long-term cost of posttraumatic knee osteoarthritis or emotional cost of a major injury to active individuals.
A successful prevention strategy must address goals of efficacy, compliance, reproducibility, and cost. Several approaches to prevention have been taken, including identifying high-risk athletes, encouraging better biomechanics, and providing structural support to a healthy knee. This chapter presents current information on concepts, strategies, and outcomes related to ACL injury prevention.
Biomechanics and the Female Athlete: The Noncontact Anterior Cruciate Ligament Injury
The first concept of ACL injury prevention begins on the tissue level and expands to include the interaction among biologic tissues and systems. A simple hypothesis would state that achieving optimal biomechanics of a tissue system would lead to a lower chance of injury to that system. The corollary argument being that less than optimal biomechanics of a tissue system would lead to a higher chance of injury to that system. Expanding this hypothesis to the competitive athlete, one would propose that well-conditioned athletes have a lower rate of injury and that poorly conditioned athletes have a higher rate of injury. More specifically, an athlete with worse biomechanics would have a greater risk of ACL injury. A dynamic, multifactorial model of sports injury etiology proposes that internal risk factors combine to make an athlete predisposed to injury. Exposure to external risk factors lead to a susceptible athlete who is then exposed to an inciting event, leading to injury (Fig. 5.1).10
What often distinguishes this injury from that of the female basketball player, however, is the presence of an external force beyond that of gravity; hence, “a contact sport.” It is thus the challenge to further define the proposed hypothesis in the context of contact versus noncontact activities. The female athlete has been used as the model for the stated hypothesis in the setting of noncontact ACL injury and, thus, is the basis for this discussion.
According to Hewett et al.,11 gender differences between male and female ACL injuries are thought to result from differences in anatomy, hormones, and neuromuscular patterns. Another study has defined these differences as nonmodifiable and modifiable.12 Nonmodifiable differences, such as femur length,13 femoral notch width,14 patient height,12 and menstrual cycle hormone levels15 16 17 contribute in different capacities to ACL injury risk. Modifiable differences, such as neuromuscular patterns, appear to result from a lack of synchronization between growth and maturity of the lower extremity and appropriate neuronal control of the lower extremity in high-risk sporting movements.18 19 20 21
ACL injury of the female athlete has typically two defining characteristics: noncontact and deceleration. Based on these characteristics, investigators have sought to understand the implications of modifiable biomechanics on female ACL injury risk patterns and the subsequent effects of
neuromuscular training designed to protect at-risk athletes. The female ACL injury risk pattern is best defined as a pathokinetic chain.22 This chain begins as an increased adductor moment at the hip leading to lower extremity valgus and, ultimately, increased ACL strain. Hewett et al.12 prescreened 205 female athletes for neuromuscular control using measurements of lower extremity joint angles and moments during a jump landing task. They noted that the nine athletes with subsequent ACL tears had an 8 degree greater abduction angle (knee valgus), 2.5 times greater abduction moment, and 20% higher ground reaction force as noted on the prescreening examinations. They concluded that landing task knee motion and loading are predictors of ACL injury risk in female athletes.
neuromuscular training designed to protect at-risk athletes. The female ACL injury risk pattern is best defined as a pathokinetic chain.22 This chain begins as an increased adductor moment at the hip leading to lower extremity valgus and, ultimately, increased ACL strain. Hewett et al.12 prescreened 205 female athletes for neuromuscular control using measurements of lower extremity joint angles and moments during a jump landing task. They noted that the nine athletes with subsequent ACL tears had an 8 degree greater abduction angle (knee valgus), 2.5 times greater abduction moment, and 20% higher ground reaction force as noted on the prescreening examinations. They concluded that landing task knee motion and loading are predictors of ACL injury risk in female athletes.
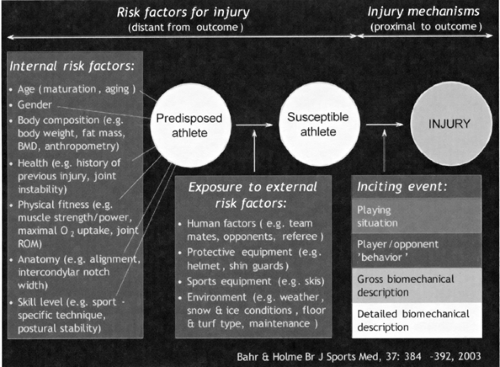 Figure 5.1. A dynamic, multifactorial model of sports injury etiology. (Adapted from Bahr R, Krosshaug T. Understanding the injury mechanisms: a key component to prevent injuries in sport. Br J Sports Med 2005;39:324–329. ) |
Other investigators have defined the at-risk position for ACL injury to be either knee varus or valgus with flexion of 10 to 30 degrees (Fig. 5.2 and Fig. 5.3).23,24 Markolf et al.25 were more specific in their study of ACL forces and specified that a varus force at the knee in combination with an internal rotation moment at the knee placed the ACL at greatest risk for tearing.
Encouraged by earlier investigations, Sell et al.26 examined gender differences in planned and reactive stop-jump tasks of different directions. Comparing 18 males with 17 females of high school age, biomechanical and neuromuscular patterns were observed in the right knee. Of the three jumping directions, lateral jumping tasks to the medial aspect of the right knee demonstrated the greatest ACL risk profile by increasing ground-reactive forces, increasing proximal tibial shear forces, increasing valgus and flexion moments, and lower flexion angles. These findings were potentiated in female athletes and by switching from a planned to a reactive task. The authors concluded that future neuromuscular and proprioceptive ACL injury prevention programs should incorporate reactive task training as well as lateral jumping strategies.
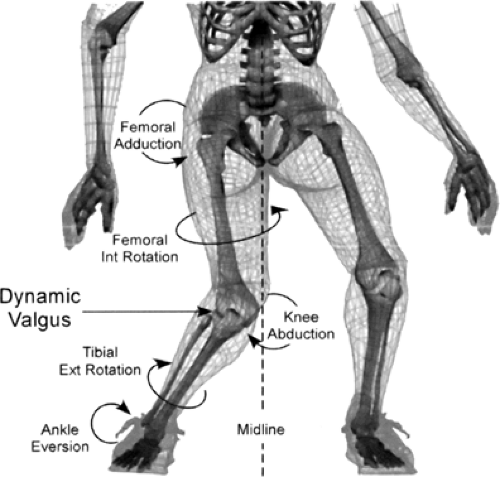 Figure 5.2. Valgus lower extremity alignment puts the anterior cruciate ligament at risk of injury. This alignment consists of hip adduction, femoral internal rotation, knee abduction, tibial external rotation, and ankle eversion. Ext, external. (Reprinted with permission from Hewett TE, Shultz SJ, Griffin LY, eds. Understanding and Preventing Noncontact ACL Injuries. Champaign, IL: Human Kinetics; 2007. ) |
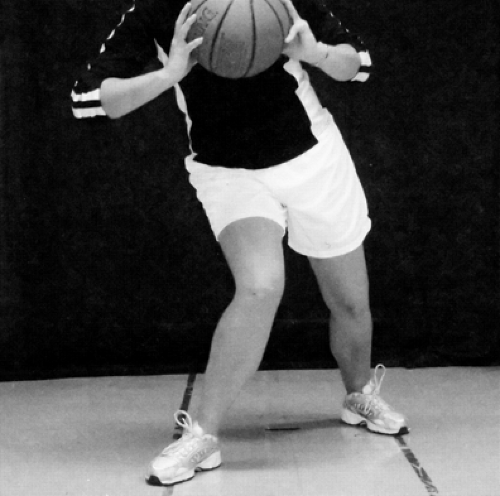 Figure 5.3. Clinical example of the valgus lower extremity at-risk alignment. (Reprinted with permission from Hewett TE, Shultz SJ, Griffin LY, eds. Understanding and Preventing Noncontact ACL Injuries. Champaign, IL: Human Kinetics; 2007. ) |
Anterior Cruciate Ligament Injury-Prevention Studies
Several ACL injury prevention studies have been performed, with many showing a reduction in the risk of noncontact ACL injury. A summary of ACL injury prevention studies is shown in Table 5.1.
Most injury-prevention schemes have focused on neuromuscular control and proprioception. Caraffa et al.3 studied 600 soccer players in Sweden. Half (300 players) were assigned proprioceptive training and the other half no training. The players were followed for three soccer seasons. The group treated with proprioceptive training demonstrated a statistically significant decrease in the rate of ACL injury compared with the untreated group.
Hewett et al.4 examined the effect of corrected jump and landing technique training on 11 female subjects (Fig. 5.4 and Fig. 5.5). They noted significantly reduced abduction moments at the knee. A similar study showed that phase-oriented and technique neuromuscular training in female athletes reduced the rate of ACL injuries to that seen in a male cohort.11 A similar risk reduction was seen in elite female
Norwegian handball players by Myklebust et al.5 In the elite players, they noted that a five-phase program of neuromuscular control and planting/landing skills significantly reduced the risk of an ACL tear over the course of two seasons. This effect was not seen in a broader skill set of female players. This led the study authors to conclude that compliance and time for training likely play a role in the success of such prevention programs. Furthermore, in a randomized trial of handball clubs in Norway, Olsen et al.27 found that a structured program of warm-up exercises to improve running, cutting, and landing technique as well as neuromuscular control, balance, and strength resulted in a reduction of knee and ankle injuries. However, a follow-up video-based intervention program studied by Arnason et al.28 did not show a reduction in ACL injury.
Norwegian handball players by Myklebust et al.5 In the elite players, they noted that a five-phase program of neuromuscular control and planting/landing skills significantly reduced the risk of an ACL tear over the course of two seasons. This effect was not seen in a broader skill set of female players. This led the study authors to conclude that compliance and time for training likely play a role in the success of such prevention programs. Furthermore, in a randomized trial of handball clubs in Norway, Olsen et al.27 found that a structured program of warm-up exercises to improve running, cutting, and landing technique as well as neuromuscular control, balance, and strength resulted in a reduction of knee and ankle injuries. However, a follow-up video-based intervention program studied by Arnason et al.28 did not show a reduction in ACL injury.
Table 5.1 Summary of Anterior Cruciate Ligament Injury-Prevention Studies | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
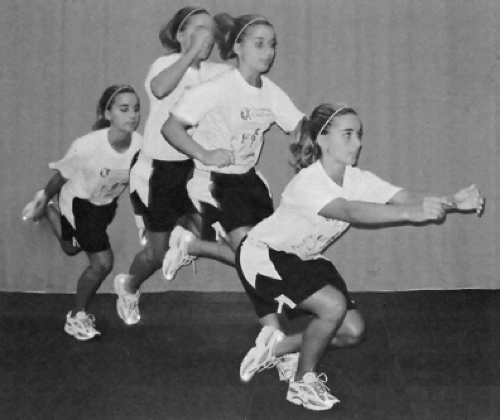 Figure 5.4. Plyometric neuromuscular training. (Reprinted with permission from Hewett TE, Shultz SJ, Griffin LY, eds. Understanding and Preventing Noncontact ACL Injuries. Champaign, IL: Human Kinetics; 2007. ) |
 Figure 5.5. Balance board training with biofeedback. (Reprinted with permission from Hewett TE, Shultz SJ, Griffin LY, eds. Understanding and Preventing Noncontact ACL Injuries. Champaign, IL: Human Kinetics; 2007. ) |
More recently, Paterno et al.29 examined the role of neuromuscular training on 41 female high school students. The intervention lasted 6 weeks and measured single-limb postural stability, anteroposterior stability, and medial-lateral stability. With focused neuromuscular training, the authors noted a significant increase in overall single-limb stability and anteroposterior stability. There was no change in medial-lateral stability. The potential for this type of neuromuscular training to reduce ACL injury in a susceptible female population will need to be determined across a larger study group.
Bracing the Intact Native Anterior Cruciate Ligament
One of the most tangible historical and current interventions for protection against ACL injury has been knee bracing. Knee braces have been developed for prophylactic, functional, and rehabilitative purposes. Support for prophylactic knee bracing (PKB) has come from athletic trainers, coaches, physicians, and, most importantly, an athlete’s family members. The effectiveness of knee bracing in protecting native ligament integrity has been studied both biomechanically and clinically.
The Biomechanical Experience
In assessing PKBs, the use of cadaveric and surrogate knee models has been viewed with skepticism. The braced knee models, while controlled, do not account for weightbearing, physiologic loads, or muscle tone. In light of these limitations, the laboratory investigations of PKBs off the playing field have provided some insight into their effectiveness in protecting against knee ligamentous injury. Further, newer laboratory methods that examine additional risk factors for noncontact injuries have led to research that accounts for the deficiencies of previous studies, including weightbearing and muscle tone.
In 1987, Paulos et al.30 published a study of 18 cadaveric knees tested with one of two lateral stabilizing braces: Anderson Knee Stabler (Vision Quest Industries, Inc., Irvine, CA [Out of Production]) or McDavid Knee Guard (McDavid Knee-Guard, Inc. Woodridge, IL). In the presence or absence of one of the lateral braces, the application of valgus force was analyzed with respect to joint line opening and resulting ligament tensions/failure. No correlation was
seen between the use of a brace and reduced joint line opening or ligament failure with application of valgus stress. The authors correlated these results to a lack of protection of the medial collateral ligament (MCL).
seen between the use of a brace and reduced joint line opening or ligament failure with application of valgus stress. The authors correlated these results to a lack of protection of the medial collateral ligament (MCL).
Also in 1987, Wojtys et al.31 focused specifically on the influence of the Lennox Hill Brace, a functional brace, in protecting the knee from excessive anterior translation or external rotation moments. The authors used four cadaveric specimens tested at 30 degrees of knee flexion to compare nonbraced and braced ligament-intact and ligament-deficient knees. Although the sample size was too small for statistical significance, the brace was noted to decrease anterior translation in the ACL intact knee and the isolated ACL-deficient knee. No effect was noted in the braced MCL-/ACL-deficient or MCL-/lateral collateral ligament-deficient knee. With regard to rotation, the brace effectively limited external rotation in all specimens regardless of ligament condition.
The variability of cadaveric knees in biomechanics testing led some research teams to test brace wear using a surrogate knee model. These models were typically made from composite materials that could be manufactured to mimic the bulk, size, and mechanics of human tissue. Additionally, some research teams employed hybrid cadaveric-surrogate knee models to capture brace effects in a reproducible and anatomic way.
Related posts:
 The ACL-Deficient Knee: Some Thoughts—Past and Future
The ACL-Deficient Knee: Some Thoughts—Past and Future
The Healing Response Technique: A Minimally Invasive Procedure to Stimulate Healing of Anterior Cruciate Ligament Injuries Using the Microfracture Technique
A Look Beyond the Horizon
Functional Biomechanics of Healthy, Anterior Cruciate Ligament-Deficient and -Reconstructed Knees
Microfracture
The ACL-Deficient Knee: Some Thoughts—Past and Future
The ACL-Deficient Knee: Some Thoughts—Past and Future
The Healing Response Technique: A Minimally Invasive Procedure to Stimulate Healing of Anterior Cruciate Ligament Injuries Using the Microfracture Technique
A Look Beyond the Horizon
Functional Biomechanics of Healthy, Anterior Cruciate Ligament-Deficient and -Reconstructed Knees
Microfracture
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


