Anorectal Malformations
David E. Wesson
Formation of the anus and rectum and separation from the urogenital tract occur primarily between the 4-mm (fourth week) and 16-mm (sixth week) stage of embryonic development but continue to the 56-mm stage. Major anorectal malformations occur in 1 per 1,500 live births. Imperforate anus does not follow a simple mendelian pattern of inheritance, although it has been reported in siblings and in members of one family over three generations.
ETIOLOGY AND CLASSIFICATION
The Hedgehog family of cell signals plays a key role in the development of the anorectal region in all vertebrate and invertebrate species. Sonic Hedgehog, an endoderm-derived signaling molecule, induces mesodermal gene expression in the hindgut of the chick embryo. Defective Hedgehog signaling in mice leads to a constellation of anomalies strikingly similar to the VACTERL (described later) association seen in humans. Mutations in Gli genes, which participate in the transduction of Hedgehog signaling, cause Palliser-Hall syndrome in humans, a prominent feature of which is imperforate anus.
Table 351.1 lists types of anorectal malformations according to gender, the level of rectal descent, and the presence or absence of a fistula. The level of rectal descent may be determined by perineal inspection or with the aid of plain radiographs, perineal ultrasound, voiding cystourethrography (VCUG), computed tomographic scanning, and magnetic resonance imaging. The traditional invertography, as described by Wangensteen and Rice, largely has been replaced by a lateral radiograph of the pelvis taken with a marker on the anal dimple and the infant in the prone position with the pelvis elevated off the bed. This study should be done more than 12 hours after birth to allow sufficient time for air to reach the rectum. If the end of the rectal air column is within 1 cm of the perineal skin, a fistula indicating a low lesion is likely to be present.
TABLE 351.1. CLASSIFICATION OF ANORECTAL MALFORMATIONS | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||
Lesions close to the anus occur more commonly than do high lesions in girls; high lesions are seen more often in boys. Nearly 80% of the boys with a high lesion have a fistula to the urinary tract, and nearly all girls with a high lesion have a cloacal anomaly (Figs. 351.1 and 351.2).
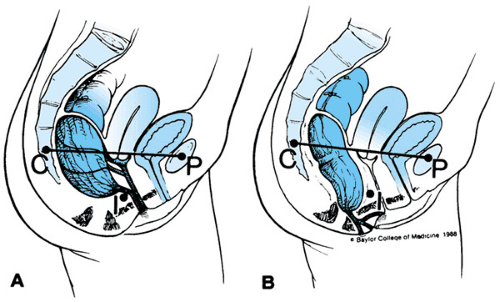 FIGURE 351.1. Anorectal anomalies in the female infant. A: High lesions usually have a cloaca, fistula to the vagina (rare), or a fistula to the vestibule. B: Low lesions also may have a fistula to the vestibule without a long shared wall with the vagina or a fistula to the fourchette or perineum. |
DIAGNOSIS
The basic steps in management of neonates with anorectal malformations are as follows:
Determine whether the level is high or low.
Check for associated defects, especially cardiac and renal.
Ensure free drainage of urine and stool.
A full assessment may require 24 to 48 hours because this length of time often is required for meconium to appear in the urine (high lesion) or perineum (low lesion). To defer any decision regarding primary repair or creation of a colostomy for at least 24 hours is wise. All patients require ultrasound screening for hydronephrosis and hydrocolpos before an operation is performed.
Several findings on physical examination suggest the level of an imperforate anus. A flat bottom with no crease or anal dimple and no evidence of an external sphincter predicts a high imperforate anus (Fig. 351.3). A prominent anal dimple not always is associated with a low anomaly. Nonetheless, a well-developed raphe, an anal dimple, and a bucket-handle deformity usually suggest a low lesion. Ninety percent of boys with a low lesion have a fistula to the perineum. Whitish inspissated mucus (perineal pearls) or meconium-stained material may be expressed from the fistula in the subcutaneous tract along the raphe of the perineum, scrotum, or even ventral surface of the penis (Fig. 351.4). Often the perineal fistula is not obvious at
birth but becomes evident with the passage of a small fleck of meconium during the first 24 hours of life (Fig. 351.5). Not all lesions with a perinela fistula are low. Boys with a flat bottom and a fistula from the rectum to the perineum greater than 1.0 cm in length may have a high lesion requiring treatment as such. The passage of flatus or meconium in the urine is diagnostic of a high anomaly with a fistula to the urethra or bladder.
birth but becomes evident with the passage of a small fleck of meconium during the first 24 hours of life (Fig. 351.5). Not all lesions with a perinela fistula are low. Boys with a flat bottom and a fistula from the rectum to the perineum greater than 1.0 cm in length may have a high lesion requiring treatment as such. The passage of flatus or meconium in the urine is diagnostic of a high anomaly with a fistula to the urethra or bladder.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


