External Fixation
Michael J. Gardner
M. Bradford Henley
Sterile Instruments/Equipment
- Large or medium external fixation system
- Open compressor/distractor device
- 4.0-mm partially threaded pins for midfoot fixation
- Towel bolsters
Positioning
- Supine on a cantilever-type, radiolucent table
- Bring patient to the cantilever (foot) end of the table
- Place small bolster (e.g., bump) under ipsilateral hip and torso
- Elevate the leg on soft ramp cushion to facilitate lateral imaging
Reduction and Implant Techniques
- Centrally threaded 5.0- or 6.0-mm pin through calcaneus for medial and lateral, “triangular” uniplanar frame.
- Medial 5.0-mm Schanz half pin for medial half-pin frame.
- Calcaneal insertion point is critical to avoid injury to lateral plantar and medial calcaneal nerves, and posterior tibial neurovascular bundle more anteriorly (Fig. 28-1).
Figure 28-1. The calcaneal pin should be placed from medial to lateral and in the posterior-inferior half of a circle that approximates the contour of the posterior tuberosity. Avoid inserting the pin into cross-hatched area. Place the pin in coronal plane. It may be inserted as either medial half pin or transcalcaneal pin. Point A: (posteroinferior medial calcaneus); Point: B (inferior medial malleolus); and Point C (navicular tuberosity). (Adapted from Casey D, McConnell T, Parekh S, et al. Percutaneous pin placement in the medial calcaneus: is anywhere safe? J Orthop Trauma. 2004;18 (8 Suppl):S39–S42. With permission.)
- Place calcaneal pin first, posteriorly and inferiorly in the tuberosity, using a lateral fluoroscopic view (Fig. 28-2).
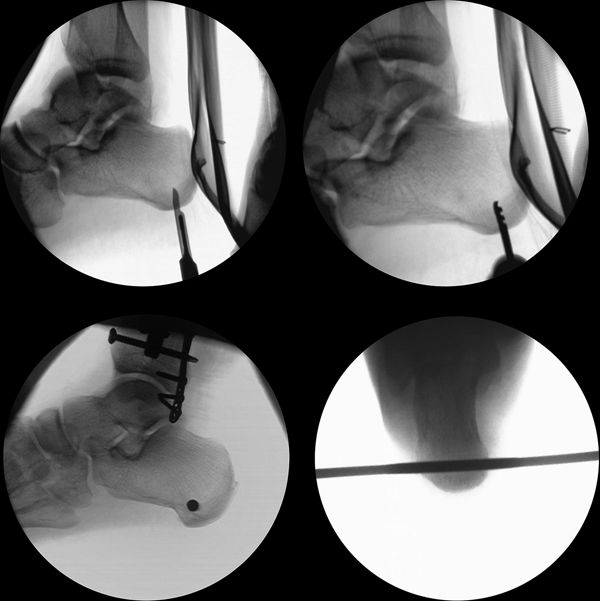
Figure 28-2. For placement of a transcalcaneal pin, the location for the incision should be estimated with a knife under fluoroscopy, and the position of the drill bit and pin should be confirmed. Ideally, the pin should be transverse on the axial view.
![]()
- If the fibula is intact or was treated with acute ORIF, the stable lateral column can be used to tension a medial frame (medial calcaneal half pin only) against the lateral fibular plate to restore limb length and angulatory alignment (Fig. 28-3).

Figure 28-3. Following fixation of the fibula, a medial frame can be used to tension against the reconstructed lateral column to restore anatomic length. An alternative to a sagittal half pin in the anterior tibia is to place a coronal half pin in the medial aspect of the proximal tibia. This configuration allows for precise control of fracture reduction, as distraction along the tibial-calcaneal bar’s axis will result in uniplanar changes. With distraction, in this example this configuration will result in multiplanar corrections (e.g., distraction and posterior translation with an additional rotational moment).
![]()
- Midfoot pin is placed from medial to lateral through the two medial cuneiforms or through all three cuneiforms.
- Because the midfoot architecture is an arch, it is important to stay in the dorsal half of the medial cuneiform, on the lateral view to avoid exiting plantarly and potentially resulting in a neural or vascular injury (Fig. 28-4).

Figure 28-4. An axial CT scan of the foot demonstrates the arch configuration of the cuneiforms (asterisks). A medial to lateral pin should enter the dorsal half of the most medial cuneiform to avoid the structures plantar to the arch (arrow).
- Use a 2.5-mm drill bit to drill a pilot hole for a 4.0 mm × 100 mm partially threaded Schanz half pin (Fig. 28-5).
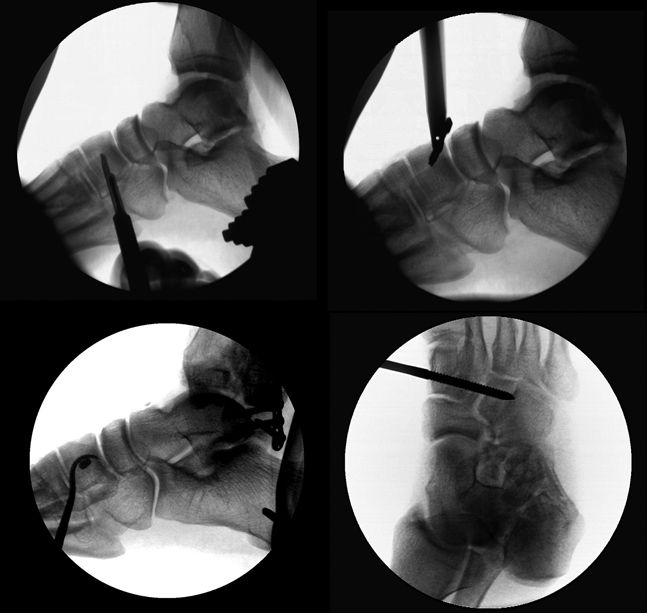
Figure 28-5. The dorsal starting point is marked with a knife, and the drill entry site and pin position are confirmed on lateral and oblique views.
![]()
- It is easier to place the midfoot pin first, prior to distracting across the ankle joint.
Related posts:

Stay updated, free articles. Join our Telegram channel



Full access? Get Clinical Tree


