Chapter 3 Anatomy review – the torso, lower limbs and feet
BONES AND JOINTS
The walls of the thoracic cage comprise the thoracic vertebral column posteriorly and the sternum anteriorly, with the ribs and costal cartilages ranged between (Fig. 3.1).
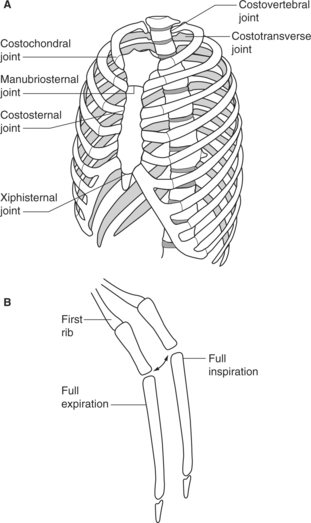
Figure 3.1 A Joints of the thorax. B Movements of the sternum during respiration (seen laterally).
Reproduced with permission from Palastanga et al (2002).
MOVEMENTS OF THE RIBS, COSTAL CARTILAGES AND STERNUM
Joint movement
The manubriosternal and xiphisternal joints are secondary cartilaginous joints between the body of the sternum, manubrium and xiphoid process. Both allow a small range of movement during breathing.
MUSCLES INVOLVED IN BREATHING
| Inspiration | Expiration |
|---|---|
| Diaphragm | Transversus abdominis |
| Scalenes | Internal obliques |
| Intercostals | External obliques |
| Levatores costarum | Latissimus dorsi |
| Serratus posterior superior | Transversus thoracis |
| Subcostals | |
| Serratus posterior inferior |
Inspiration
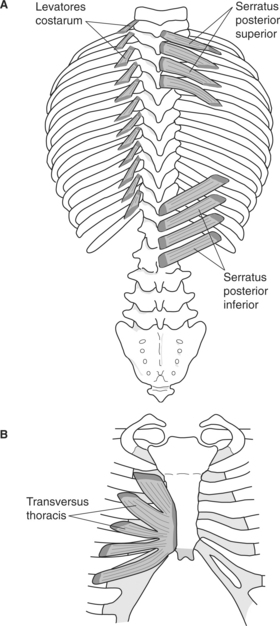
The diaphragm is a dome-shaped musculotendinous leaf separating the thoracic and abdominal cavities (Fig. 3.2). It has several major points of origin around its circumference: the xiphoid process; the deep surfaces and cartilages of the seventh to the twelfth ribs; the lumbar vertebrae via the ‘right crus’ and ‘left crus’, ligaments that arise from the bodies of the lumbar vertebrae L1–L3 and L1–L2, respectively; and the arcuate ligaments that attach to the lumbar vertebrae.
Expiration
The subcostals are muscle slips found mainly in the thoracic region lying between the ribs across two intercostal spaces. They assist in lowering the ribs and producing expiration.
‘Serratus posterior inferior lies deep to latissimus dorsi, arising from the spinous processes T11, T12, L1 and L2 and their supraspinous ligaments via the thoracolumbar fascia. It helps to pull the lower four ribs downwards and backwards’ (Palastanga et al 2002, p. 483).
In normal breathing
 During inspiration the abdominal muscles relax and reduce intra-abdominal pressure, allowing the diaphragm to lower as it contracts.
During inspiration the abdominal muscles relax and reduce intra-abdominal pressure, allowing the diaphragm to lower as it contracts.
In forced expiration
 The abdominal muscles actively contract and further increase intra-abdominal pressure as the diaphragm relaxes. This pushes the abdominal contents against the diaphragm, increasing its upward displacement as it ascends. This in turn increases intrathoracic pressure that forcefully compresses and deflates the lungs.
The abdominal muscles actively contract and further increase intra-abdominal pressure as the diaphragm relaxes. This pushes the abdominal contents against the diaphragm, increasing its upward displacement as it ascends. This in turn increases intrathoracic pressure that forcefully compresses and deflates the lungs.
MOVEMENTS OF THE VERTEBRAL COLUMN AND THE MAIN MUSCLES INVOLVED
Cervical spine
Lumbar spine
Flexion and extension
Psoas major and the anterior abdominal wall muscles control extension from the upright position; from the prone position the postvertebral muscles, assisted by quadratus lumborum contracting bilaterally, produce it. Quadratus lumborum also assists lateral stability as the lumbar spine extends (Palastanga et al 2002, p. 512).
Thoracic and lumbar spine
Lateral flexion and rotation
The spinal muscles can also produce lateral flexion, erector spinae contracting unilaterally to produce lateral flexion with rotation to the side of the contraction and multifidus producing lateral flexion as well as extension and rotation at all levels of the vertebral column. Additionally, intertransversarii found in the cervical and lumbar regions can contract unilaterally to produce lateral flexion on the side of the contraction; however, both intertransversarii and multifidus act more importantly as stabilizers of the vertebral column during lateral flexion.
BONES AND JOINTS
In children between the ages of 2 and 13 years the lumbosacral joint is very mobile and provides up to 75% of the total range of flexion and extension of the lumbar spine. However, this mobility reduces during puberty and adulthood so that by 35 years of age the average range of flexion and extension available is approximately 18 degrees and this reduces further as people age. Lumbosacral mobility in lateral flexion is considerably less than in flexion and extension, being approximately 7 degrees in children, 1 degree in mature adults and absent in the elderly.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


