Fig. 1.1
This drawing shows the two major bones of the lower extremity: the tibia and the fibula. It gives an overview of all the different structures located on these two bones, mostly focused on the posterior surface. In addition, origins of muscles are labeled to illustrate where the major muscles of the posterior lower leg originate
The shaft of the tibia consists of a medial, a lateral, and a posterior surface. The anteromedial surface of the tibia or “shin” is subcutaneous and easily palpated in most people. Whereas the anteromedial part of the tibia has virtually no attachments, the posterior part has a significant number of attachments: semimembranous, popliteus, soleus , tibialis posterior , and flexor digitorum longus (the vertical line separates the two latter muscles). The posterior surface of the tibia includes muscular attachments relevant to muscular injuries of the posterior leg . In general, the flexor muscles are attached to the posterior part of the tibial shaft [2]. The posterior surface is bound by the interosseous and medial borders of the tibia. Both the soleal line and the vertical line are located on the posterior surface. The distal end of the tibia articulates with the fibula and talus to form the ankle joint. The distal tibia consists of a number of different surfaces: anterior, medial, posterior, lateral, and distal. The most distal aspect of the tibia is the medial malleolus, just lateral to this is the groove for the tibialis posterior tendon.
Running posterolateral to the tibia, the fibula is the thinner and weaker of the two leg bones. The fibula does not articulate with the femur and has a limited role in weight bearing. It is the site of the distal muscular attachment of the biceps femoris and muscular origin of several muscles of the leg. It begins proximally at the fibular head, an easily palpated structure found just posterolateral to the lateral tibial plateau. The fibula head is an important landmark because this is the location to which a number of clinically significant structures attach: extensor digitorum longus and peroneus longus and soleus, as well as the fibular collateral ligament, or lateral collateral ligament (LCL), connected to the biceps femoris. Below the head, the fibula consists of a shaft and the lateral malleolus, also known as the distal end of the fibula. The shaft has three surfaces and borders: anterior, posterior, and interosseous. The posterior surface is the largest of these and includes muscular attachments for the tibialis posterior, soleus , flexor hallucis longus, peroneus longus, and peroneus brevis, while the anterior surface includes attachments for the extensor digitorum longus and extensor hallucis longus [3]. Please see Fig. 1.1 for illustration of the mentioned bony structures and attachments.
Soft Tissue Structures of the Leg
In the leg, as throughout the limbs, functionally related groups of muscles are contained in fascial compartments . These compartments are bound by a thick canvas-like covering of deep fascia and share a neurovascular supply. The soft tissues of the leg are divided into four of these compartments: the anterior, the lateral, the superficial posterior, and the deep posterior. These four compartments are divided by crural (leg) fascia, also called fascia cruris, which is the deep fascia of the lower leg; more posterior, it is known as the popliteal fascia.
Although the main focus of this book is on the muscles of the superficial and the deep posterior compartments , the proximity of the lateral and posterior compartments as well as their functional overlap necessitates careful delineation of lateral and posterior compartments clinically. The lateral compartment houses several clinically important structures, including the common peroneal nerve, the peroneus longus, and the peroneus brevis. The peroneus longus is the more superficial of the two muscles; it everts and plantarflexes the foot (Fig. 1.2) [3].

Fig. 1.2
This picture, taken in the anatomy laboratory, illustrates the location of the peroneus longus and the peroneus brevis muscles and their location in relation to the fibula and some of the other structures of the posterior leg such as the soleus and the tibial nerve
The most distal part of this peroneus longus consists of a very long tendon. The peroneus brevis is located just anterior to the peroneus longus. The common peroneal nerve moves from its proximal posterior location behind the fibular head to an anterior lateral position as it transverses between the fibular head and shaft. Both muscles are supplied by the superficial peroneal nerve, which also provides sensory innervation to the dorsum of the foot.
The superficial posterior compartment consists of the gastrocnemius , soleus, plantaris, and tendo calcaneus (Achilles tendon) . As a functional unit, the superficial posterior compartment is critical in maintaining functions of standing posture and gait. As a group, they primarily assist in flexing the knee and plantarflexing the foot.
The gastrocnemius is the largest and most superficial muscle of the superficial posterior compartment. Its heart-shaped landmarks are easily visible through the skin in well-trained athletes. The more proximal part of the gastrocnemius (its “belly”) originates from two heads, which are connected to the femoral condyles by tendons. More specifically, there is a medial and a lateral head. The medial head tends to be the larger of the two. On its distal end, the muscle becomes narrower and blends to form a union with the Achilles tendon. Starting above the knee and extending beyond the ankle to the calcaneus, the gastrocnemius crosses two joints. This biarthodial architecture conveys a unique functional continuity with the hamstrings in initiating knee flexion and limiting knee extension. Rarely, individuals may not have a lateral head of the gastrocnemius , or a third head may be present [5]. The tibial nerve provides the innervation of the gastrocnemius.
The soleus , located just deep or anterior to the gastrocnemius, is a broad and flat muscle. The soleus has a central tendon and pennate structure. Unlike the gastrocnemius, which spans two joints (the knee and the ankle), the soleus originates on the posterior tibia and crosses only the ankle joint. It is attached proximally to the posterior border of the tibia and fibula by an arch-like aponeurosis with a tendinous gap centrally. The posterior tibial artery and tibial nerve pass through this gap to enter the deep posterior compartment . The more distal end of the muscle connects to the gastrocnemius, which then, as noted above, forms the Achilles tendon . As a result, there is a strong synergistic relationship between the gastrocnemius, the soleus, and the Achilles tendon, which is important in regard to the injuries discussed in the following chapters. Please see Figs. 1.3 and 1.4 for illustration of the mentioned muscles.

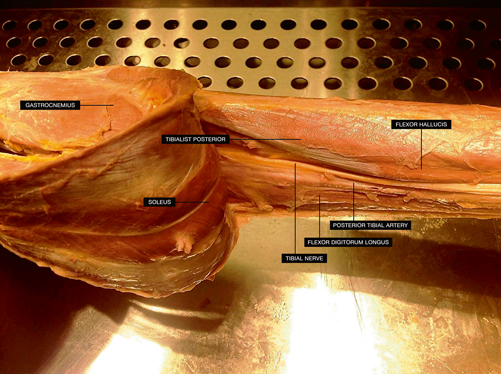
Fig. 1.3
Another picture taken in the anatomy laboratory illustrating the strong relationship between the gastrocnemius muscle and the calcaneal tendon
Fig. 1.4
This image shows the location of the soleus, a broad and flat muscle, found deep to the gastrocnemius. In addition, the tibial nerve is labeled, innervating both the gastrocnemius and the soleus
The soleus has a high percentage of fatigue-resistant muscle fibers and plays a critical role in maintaining standing posture and walking gait. The soleus muscle is supplied by two branches of the tibial nerve. Accessory soleus muscles are well-known but uncommon congenital anomaly [6]. An accessory soleus can be a source of exertional pain due to an inadequate blood supply from the posterior tibial artery.
The plantaris is a rather small muscle and actually has been found absent in a number of individuals. It originates from the lateral supracondylar line deep to the lateral head of the gastrocnemius . From this lateral attachment on the femur, it moves medial as it extends distal. The muscle ends shortly after crossing the knee joint, where at approximately the origin of the soleus, it transitions in a long, thin tendon that traverses between the medial head of the gastrocnemius and the soleus before inserting on the medial calcaneus either independently or by means of the Achilles tendon . In the setting of an Achilles tendon rupture and a preserved independent attachment of the plantaris tendon to the calcaneus, the ability to plantarflex the ankle can remain potentially confounding for the clinical diagnosis. The plantaris is supplied by the tibial nerve. It is referred to by some as the gastrocnemius’s “little helper,” as it acts in conjunction with the gastrocnemius in an accessory fashion. Like the gastrocnemius, it crosses both the knee and ankle but due to its small size and absence in some individuals, the functional role of the plantaris is traditionally thought to be relatively insignificant and it is considered by many to be a vestigial muscle. Indeed, the plantaris tendon is harvested for autograph tendon repair for this very reason [7]. However, the pattern of a small muscle running in parallel with a larger prime mover has been termed parallel muscle combination, and in these combinations the small muscle has been found to have a high density of muscle spindles. Some authors have proposed these muscles may serve an important proprioceptive function, providing neurologic feedback to regulate movement [8]. It should be noted that discussion regarding the function of the plantaris can be influenced by larger arguments regarding the implications of vestigial muscle as evidence for evolution [9].
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


