Muscle
Muscle belly length (cm)
Fiber length (cm)
Pennation angle (deg)
Fiber arrangement
ST
26.8 ± 3.6
23.8 ± 1.8
0
Parallel fibered muscle
G
24.9 ± 2.4
24.3 ± 1.9
0
SM
28.5 ± 2.6
6.0 ± 0.8
31 ± 5
Unipennate muscle
BF
31.2 ± 5.2
7.3 ± 1.3
28 ± 4
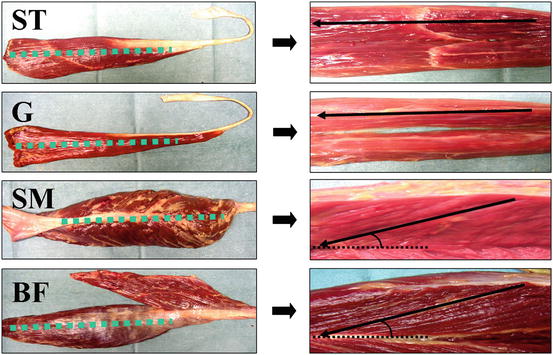
Fig. 24.1
Typical examples of knee flexor muscles from a human cadaver. The pictures on the right show the fiber arrangement visualized after incision along the dotted lines in the left
24.3.2 In-vivo Clinical Study
No significant differences were measured in the peak isokinetic flexion torque or the peak torque angle between the normal and the ACL reconstructed limbs. However, differences in isokinetic torque appeared as the knee flexion angle increased. The torque of the ACL reconstructed limb was significantly lower than that of the normal limb at 60°, 75°, 90°, and 105° of knee flexion (p < 0.05 at 60°, p < 0.01 at 75°, 90°, and 105°). The differences were not significant at 15°, 30°, or 45° (Fig. 24.2). The isometric torque of the ACL reconstructed limb at 45° (130 ± 23 % of body weight: %BW) was not significantly different from that of the normal limb (123 ± 22 %BW), however at 90°, the torque of the ACL reconstructed limb (55 ± 19 %BW) was significantly lower than that of the normal limb (88 ± 28 %BW, p < 0.01).
Fig. 24.2
Isokinetic torque at sequential 15° increases in knee flexion angle *: p < 0.05, **: p < 0.01; a comparison between normal and ACL reconstructed limbs
During the 50 % MVC, the I-EMG value for the SM and BF of both limbs was significantly reduced as the knee flexion angle increased (p < 0.01) (Fig. 24.3a, b). For the ST, the I-EMG value for the normal limb did not change while the value for the ACL reconstructed limb significantly decreased from 45° to 90° of knee flexion (p < 0.01) (Fig. 24.3c). The I-EMG value at 90° for each muscle and for each limb is calculated as a percent of the I-EMG value at 45° and shown in Fig. 24.3d. The I-EMG values for the SM and BF of both limbs at 90° were significantly reduced to approximately 65 % of the values at 45° (p < 0.01). In addition, no significant differences were found between the normal and ACL reconstructed limbs in the SM and BF. However, for the ST a significant difference was found between the limbs (p < 0.05). The I-EMG value at 90° in the normal limb was 108.5 ± 56.0 % of the value at 45° (p > 0.05), while in the ACL reconstructed limb, the I-EMG value significantly decreased to 70.4 ± 29.6 % of the value at 45° (p < 0.01).
Fig. 24.3
I-EMG value of the SM (a), BF (b), and ST (c) **: p < 0.01 compared with the value at 45°. (d) I-EMG value at 90° calculated as a percentage of the I-EMG value at 45°. #: p < 0.05, **: p < 0.01 compared with the value at 45°
The volume of the ST calculated from the MRI images was significantly smaller in the ACL reconstructed limb (68.7 ± 17.4 %) than in the normal limb (p < 0.01), whereas the volumes of the SM and BF were not different between the limbs. In all subjects, regeneration of the ST tendon was confirmed. Since the regenerated tendon passed the knee joint and inserted into a structure distal to the knee, it could function as a knee flexor. The ST musculotendinous junction in the reconstructed limb in almost all subjects was located more proximally from the knee joint space than that in the normal limb. In only one subject did the musculotendinous junction of the reconstructed limb appear in the same image as the normal limb. The difference in location between the limbs ranged from 0 to 5 images, which corresponds to a distance of 0–6 cm.
24.4 Discussion
In agreement with studies by Lipscomb et al. (1982) and Maeda et al. (1996), we found that after ACL reconstruction using the ST or STG tendon, the peak knee flexion torque of the ACL reconstructed limb that was measured at approximately 20° of knee flexion had recovered to 96 % of that of the normal limb. However, significant differences in knee flexor strength between the normal and ACL reconstructed limbs both in isokinetic and isometric contraction were found at angles of knee flexion greater than 60°. This result is similar to the finding of Tashiro et al. (2003).
From the anatomical study, considerable differences in the muscle architecture of each knee flexor muscle were shown. The ST and G were parallel fibered muscles with long fiber lengths. Thus, the number of sarcomeres in series is large for these muscles which illustrates an eminent potential for the ST and G to shorten at long distances. On the other hand, the SM and BF were unipennate muscles, characterized by short fiber lengths and a pennation angle that increases with increasing knee flexion angles. These features suggest that the SM and BF are insufficient to produce knee flexion torque at deeper angles. As results from our EMG analysis indicate, these architectural differences seem to reflect functional differences between the ST and the SM and BF. Therefore, it appears that the SM and BF cannot compensate for the function of the ST, particularly at deep flexion angles. We believe that the ST plays an important role at over 60° of knee flexion, while the SM and BF work together to produce the peak knee flexion torque occurring at less angles, since no significant difference of the peak torque and peak torque angle between the normal and reconstructed limbs were measured in the present study. Furthermore, since the G is a parallel fibered muscle with a long fiber length, it may compensate for the function of the harvested ST and should be preserved in ACL reconstruction. In fact, Tashiro et al. (2003) have reported that the reduction of the flexion torque at 70° of knee flexion and beyond was more often observed in patients with ACL reconstruction using the ST and G tendon than in patients where only the ST was used for reconstruction.
In this study, regeneration of the ST tendon was confirmed in all subjects. Previously, Eriksson et al. (1999) and Rispoli et al. (2001) confirmed regeneration of the ST tendon in MRI images taken at the level of the tibial plateau and superior pole of the patella, respectively. In addition to the regenerated tendon, we were able to measure the location of the ST musculotendinous junction by analyzing the MRI images in sequence from the knee joint space level and found that the musculotendinous junction of the ACL reconstructed limb shifted proximally as compared to that of the normal limb. Similarly, Papandrea et al. used ultrasonography (Papandrea et al. 2000) to show that the insertion of the regenerated ST tendon was proximal to that of the normal tendon. Our results also showed that the volume of the ST after its tendon was harvested for ACL reconstruction was significantly smaller than the normal ST. However, the volume of the SM and BF did not change significantly. As in the results from our EMG study, these architectural changes, such as atrophy and shortening of the ST in the ACL constructed limb, seem to have an effect on knee function at deep knee angles. Although the ST tendon had regenerated in all subjects, the regenerated ST tendon probably did not function in the same manner as in the intact (i.e., native) tendon.
Related posts:
 Injury and Illness Surveillance Among Olympic Athletes: Summary of the 2010 Winter, and the 2008 and 2012 Summer Olympic Games
Injury and Illness Surveillance Among Olympic Athletes: Summary of the 2010 Winter, and the 2008 and 2012 Summer Olympic Games
 Anterior Cruciate Ligament Injury Prevention in Female Adolescents
Anterior Cruciate Ligament Injury Prevention in Female Adolescents
 Anterior Cruciate Ligament Injury Prevention in Female Lacrosse Players Based on an Examination of Knee and Hip Joint Mechanics During Drop Vertical Jumps Performed While Holding a Lacrosse Stick
Anterior Cruciate Ligament Injury Prevention in Female Lacrosse Players Based on an Examination of Knee and Hip Joint Mechanics During Drop Vertical Jumps Performed While Holding a Lacrosse Stick
 Kinematics of the Foot and Ankle
Kinematics of the Foot and Ankle
 Prevention of Head and Neck Trauma in Rugby
Prevention of Head and Neck Trauma in Rugby
 Electromyographic Analysis of Deep Trunk Muscles During Sports Activities
Electromyographic Analysis of Deep Trunk Muscles During Sports Activities
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


