CHAPTER 30 Agee Endoscopic Carpal Tunnel Release
Introduction
In 1989, Chow et al. described a two-portal endoscopic carpal tunnel release (ECTR) technique.1 This method has undergone a number of modifications since that time and is described in a separate chapter. Agee et al. published a prospective randomized clinical trial on his uniportal technique in 1992.2 Other investigators have published their preferred technique of using a one- or two-portal approach. The decision as to which technique to use is largely based on personal preference and comfort with the procedure. This chapter discusses the uniportal technique using the Agee endoscope.
Contraindications
Absolute contraindications include any distortion of the carpal canal due to tumor, previous surgery, carpal fracture/dislocation, or mal-union of the radius. A loss of wrist extension of 20 to 30 degrees either from bony fusion or wrist contracture would hamper this procedure by impeding the correct placement of the endosocope. Unfamiliarity with the regional anatomy is another contraindication. Due to the high learning curve, it is recommended that anyone contemplating this procedure should take a cadaver training course prior to attempting it clinically—unless training has been provided in a teaching environment.3
Relative contraindications abound and are not universally agreed upon. Flexor tendon thickening due to synovial hyperplasia or adhesions from previous flexor tendon repairs will complicate the procedure. Recurrent or persistent carpal tunnel syndrome following a previous release often includes a component of traction neuropathy due to scar, which may thwart attempts at ECTR. However, successful cases have been reported.4 Any suspicion of separate entrapment of the recurrent motor branch mandates an open procedure.
Relevant Anatomy
The flexor retinaculum (FR) consists of three distinct and continuous segments that extend from the distal radius to the base of the long finger metacarpal.5 The proximal segment is continuous with the deep forearm fascia and is inseparable from the thickened antebrachial fascia. The transverse carpal ligament (TCL) makes up the second part of the FR. The TCL arises from the scaphoid tuberosity and trapezial beak radially, and from the pisiform and hook of the hamate ulnarly. The distal segment of the FR consists of the aponeurosis between the thenar and hypothenar muscles. The median nerve becomes superficial in the forearm approximately 5 cm proximal to the wrist. It lies between the tendons of the flexor digitorum superficialis (FDS) and the flexor carpi radialis (FCR), and is dorsal or dorsoradial to the palmaris longus (PL).
Surgical Considerations
The position of the ulnar nerve and artery are of particular significance for endoscopic carpal tunnel release. Most endoscopic devices are designed to divide the flexor retinaculum just to the radial aspect of the hamate hook. In an anatomical study of the boundaries of Guyon’s canal, however, Cobb et al. showed that the confines of this space do not extend from the pisiform to the hook of the hamate (as previously accepted).6 The fascial roof extends radial to the hook of the hamate, which allows the ulnar neurovascular bundle to course radial to the hamate hook. Utilizing cross-sectional analysis of nine cadaver specimens, they found the ulnar artery to course radial to the hamate hook in five and palmar to it in four. Therefore, the ulnar artery may be at greater risk of injury during endoscopic procedures than previously recognized.
The safest path for release of the TCL has been studied extensively. Rotman and Manske investigated the anatomical relationships of an endoscopic carpal tunnel device to surrounding soft-tissue structures along the ring finger and the long-ring interspace axis.7 The average distance from the center of the device to the median nerve in the carpal tunnel averaged 3.3 mm in the ring finger axis and 2.5 mm in the long-ring interspace axis. The average distance from the distal edge of the transverse carpal ligament to the superficial palmar arch was 4.8 mm in the ring finger axis and 5.5 mm in the long-ring interspace axis. These and other more subtle anatomical observations indicate the greater safety of using the ring finger axis for endoscopic carpal tunnel release.
Surgical Technique
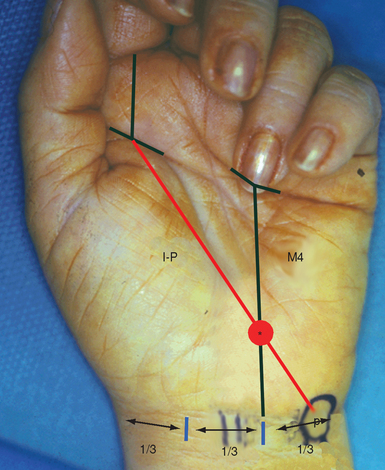
The landmarks to localize the hook of the hamate are as follows.8,9 First, the pisiform is palpated and marked. A second mark is placed on the proximal palmar skin crease, in line with the mid portion of the index finger. These two points are then connected, forming the index-pisiform line. A second line is drawn from the midpoint of the base of the ring finger, proximally to the wrist crease at the junction of its middle and ulnar third—forming the fourth metacarpal line. The intersection of the index-pisiform line and the fourth metacarpal line directly overlies the hook of the hamate (Figure 30.1). The palmar longus tendon (if present) is traced. The dissection should stay medial to the PL, which protects the median nerve.
< div class='tao-gold-member'>
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


