Adult Degenerative Scoliosis
Paul A. Lotke
Malcolm L. Ecker
 A 74-year-old male with long-standing recurrent episodes of low back pain (LBP) has noted occasional radiation into his buttocks, posterior calf, and lateral foot. His symptoms have relapsed and recurred over many years. He was able to function reasonably well with restricted activity but never pain free. His past 6 months have been extremely uncomfortable, and he has not had any relief. Pain is in his back with burning pain into his thigh. Anti-inflammatory medication has been minimally effective, and he resists narcotic medication. His x-rays and magnetic resonance imaging (MRI) show severe multilevel involvement. |
CLINICAL PRESENTATION
Adult degenerative scoliosis is a complex problem created by the combination of degeneration of the disks, arthritis in the facet joints, and osteoporosis. Asymmetric forces cause the vertebrae to unevenly settle upon themselves, rotate, and create a spinal curvature (Fig. 4-1). The curvature creates increasing asymmetric forces on the concave part of the curve. As the curve increases, the forces increase and accelerate the process. Commonly there is an associated loss of the normal lumbar lordosis producing the flat back syndrome. The patients prefer walking flexed and lean on their shopping carts (shopping cart sign), and attempts at walking upright cause anterior groin pain from hyperextension of the hips and increased back pain. The shopping cart sign may also be seen to relieve pseudoclaudication from spinal stenosis.
Each segment of the spine includes two facets, posterior and the disk anterior. Each of these structures can develop degenerative changes. If there are asymmetric degenerative changes in the facts and asymmetric collapse of the disk, this results in a lateral angulation, rotational deformity, and increasing relative kyphosis. Secondary hypertrophic changes can create stenosis in the foramina and central recesses.
This problem is associated with aging, and it usually occurs in patients over 65 years of age, but the process was initiated well before that age. Predisposing factors may include previous back injury, herniated disks, prior back surgery, and osteoporosis. It may be more common in women and may have a familial, genetic basis.
The history will reveal intermittent episodes of significant low back pain that progresses over decades and gradually creates increasing disability. The pain may be localized to the low back initially. However, with increasing structural change and curvature, there will be nerve root irritation, creating symptoms in the leg and/or foot. These may include pain radiating into the buttock or legs with activity, numbness, burning, or weakness. The radiating symptoms vary with the nerve roots affected. Unfortunately, the problem may be widespread, involve several lumbar vertebrae, and create a spectrum of symptoms that are difficult to localize. The most frequently involved segments are from the L4-5 distribution, usually on the concave side. In addition, narrowing of the central canal produces spinal stenosis with the additional symptomatology of pseudoclaudication.
CLINICAL POINTS
Elderly
Progressive
Structural changes including loss of lumbar lordosis
Height reduction
Rib impingement to iliac crests
Diffuse symptoms in low back, buttocks, and legs
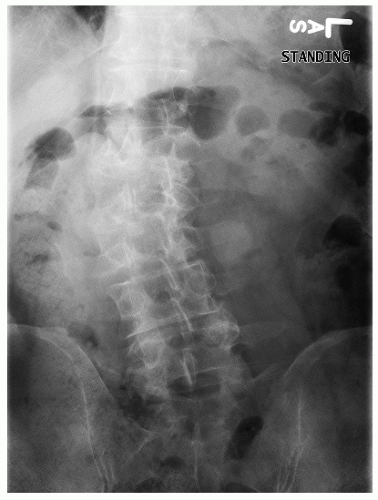 FIGURE 4-1. AP standing x-ray showing diffuse degenerative changes and scoliosis in lumbar spine. |
PHYSICAL FINDINGS
The physical examination may vary from minimal changes to marked deformity of the spine. Findings may include a list to one side, palpable curvature of spinal processes, loss of lumbar lordosis, diminishing height, and lower ribs settling closer to the iliac crests. Neurologic findings may occur with increasing nerve root irritation and depend on the level of maximal involvement.
 FIGURE 4-2. Computed axial tomography (CAT) scan shows significant degenerative changes in facet joint and disk. |
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


