Hip Pain in the Young: Femoroacetabular Impingement (FAI)
Kristofer J. Jones
Charles L. Nelson
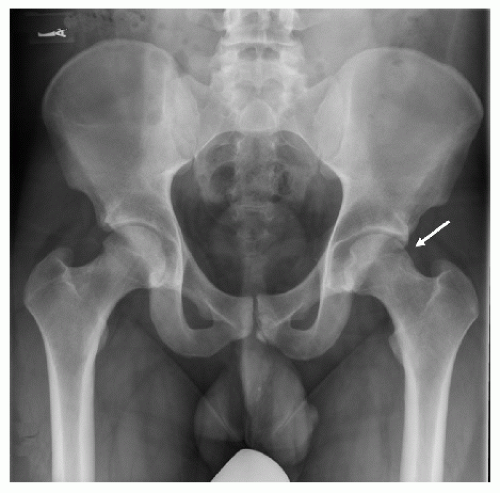 A 31-year-old man reports left anterolateral hip pain of gradual onset during the past year that has significantly limited his ability to run and exercise. He characterizes the pain as a “sharp, stabbing” sensation that is exacerbated with any pivoting activities. He cannot recall any preceding traumatic injury to the area and states that he has been taking six to eight ibuprofen tablets per day, which has provided no relief. An anteroposterior (AP) radiograph demonstrates a cam lesion of the left femoral head (arrow). Appropriate evaluation and management of this patient is discussed in this section. |
CLINICAL PRESENTATION
Femoroacetabular impingement (FAI) refers to abnormal contact of the femoral head or neck against the acetabular rim during hip range of motion. Individual predisposition for FAI can be related to specific osseous abnormalities, which can be congenital or developmental in nature. Two distinct types of impingement have been described based upon the location of the bony abnormalities and are referred to as cam or pincer impingement. Cam impingement refers to bony overgrowth at the femoral head-neck junction that results in increased radius of the femoral head and subsequent abnormal abutment of the femur against the acetabulum during hip flexion. This type of impingement is more common in the young, adult male. Pincer impingement refers to excessive overhang of the anterior acetabulum that results in abnormal contact between the femoral head and acetabulum and is commonly observed in athletic, middle-aged women (Fig. 10-1).
Typically, patients with FAI complain of anterolateral hip and/or groin pain that is exacerbated with activities that require deep hip flexion. They characterize the pain as a “sharp, stabbing pain” or a “dull ache” that may be intermittent in its initial stages but gradually progresses with time. Patients often complain of pain with prolonged sitting, rising from a seat, getting in or out of a car, and leaning forward. Mechanical symptoms (locking, catching, and/or clicking) may accompany the pain and serve as an important clue to the diagnosis, as they may represent a secondary labral tear that has occurred due to the abnormal contact between the femoral head and acetabulum. In recent years, FAI has been associated with a number of hip conditions including slipped capital femoral epiphysis, Legg-Calve-Perthes disease, and previous femoral neck fracture. Upon presentation, it is important to obtain any information about preexisting hip disease or trauma as a child or young adult.
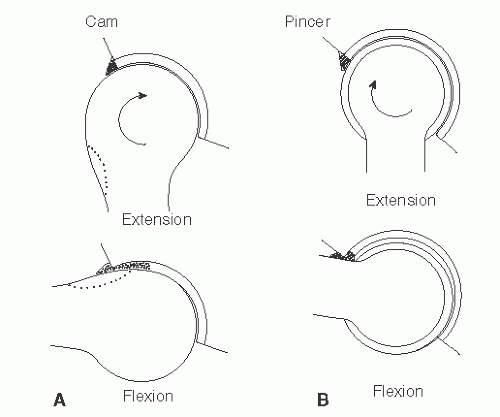 FIGURE 10-1. In cam impingement (A), an enlarged femoral head-neck junction (represented by dotted lines) results in impingement on the acetabular rim in flexion. In pincer impingement (B), overcoverage of the femoral head by the anterior region of the acetabulum can cause abnormal contact during hip flexion. |
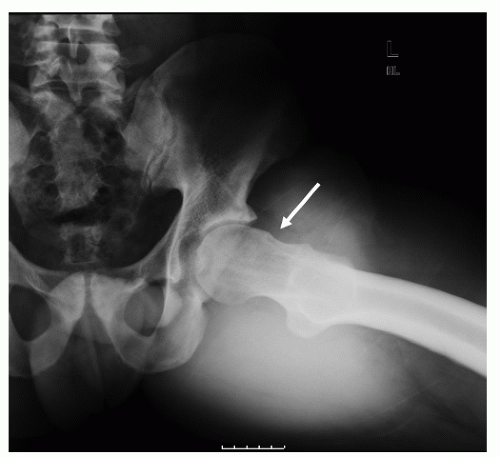 FIGURE 10-2. Frog-leg lateral view of the left hip demonstrates a focal bony prominence of the femoral head-neck junction consistent with a cam lesion. |
 FIGURE 10-3. Coronal T1-weighted image demonstrates focal bony prominence at the femoral head-neck junction (white arrow) and a degenerative anterosuperior labrum (red arrow).
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
