Chapter 17 Acute joint pain
Case 17.1
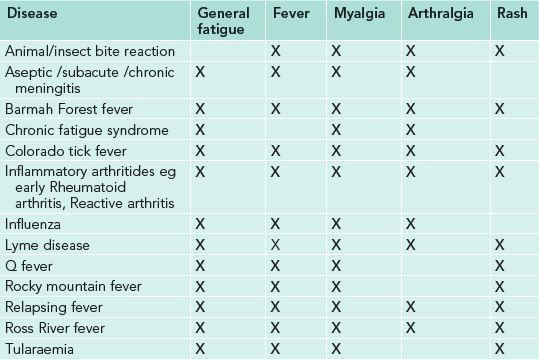
Lyme disease is the most likely diagnosis.
This disorder usually manifests itself as a localised infection of the skin (erythema migrans), followed by multiple spirochete reactions on the skin and body parts such as the heart, joints and nervous system. The disease is divided into three stages.[1]
Case 17.2
The fact that only one joint is involved, and there is no prior history of similar attacks in the knee or any other joints, makes the differential diagnoses of gout and RA less likely; the first onset of either of these in the knee would be an uncommon presentation. Gout is most common in the first metatarsophalangeal joint, while RA most commonly presents initially in the small joints of the hands or feet. In contrast, the knee is the most common site of presentation for septic arthritis and CPPD. The fact that the patient feels generally well and denies fever makes septic arthritis somewhat less likely, and he is a little young compared to the common age of onset for CPPD. First onset of RA is generally considered to be most common at a younger age than in this patient, however, a shift towards a more elderly age of onset has been noted in a recent review of epidemiological studies.[2] The description of the onset of his pain, however, seems consistent with ‘crescendo pain’ (pain which peaks over 6–12 hours from onset), which is typical, but not specific, of gout.[3] There is no clear ‘most likely’ diagnosis for this patient at this point.
The physical examination should focus on the involved knee and its surrounding soft tissues, with a comparison to the opposite knee and a screening of other joints for involvement. A more general examination of the patient should also be undertaken to assess for systemic manifestations of disease.[5]
The presentation of an acute attack of joint swelling, with overlying erythema and the description of ‘crescendo pain’, is highly suggestive of crystal inflammation.[3] This, together with the lack of other joint involvement, and no signs of systemic illness, make gout or CPPD more likely than RA or septic arthritis.
Both hypertension and a high BMI have been identified as significant risk factors for the development of gout.[2] The presence of tophi suggests longstanding hyperuricemia and would not normally be seen in a presentation of acute gout, therefore their absence does not affect the differential diagnosis.
The absence of X-ray findings is common in acute gout, and this does not therefore exclude it as a diagnosis.[3] Similarly, early in the onset of RA and septic arthritis there are often no bony changes visualised on X-ray. In CPPD you would normally expect to see linear opacification of articular cartilage (chondrocalcinosis) so this differential is now less likely. On the basis of all the history and examination findings so far, acute gout seems the most likely diagnosis.
In typical presentations of gout (ie: recurrent podagra with hyperuricaemia) a clinical diagnosis alone is reasonably accurate but not definitive without crystal confirmation.[3] However, since this is not a typical area of presentation for gout, further investigations would be required. The joint should be aspirated to allow analysis of the synovial fluid for appearance, presence of urate crystals, leukocyte count and differential, gram staining, and culture to help confirm the diagnosis. Recently the use of high-resolution ultrasonography has shown to be useful in the early diagnosis of gout,[6] CPPD[7] and RA,[8] and may well become the imaging modality of choice in the future for the investigation of an acute monoarthritis.
Chronic joint pain and restricted range of motion are common sequelae of septic arthritis, but a delay in diagnosis can result in bacteraemia, sepsis, joint destruction and even death. Therefore it has been suggested that an acute monoarticular arthritis is treated as ‘septic until proven otherwise’.[9]
The blood pressure reading of 145/95 would be classified as grade 1 (mild) hypertension if it is maintained at this level with repeated readings. Since this patient has no cardiovascular complications, target organ damage, or diabetes, his blood pressure should be remeasured monthly and referred to his general practitioner if the reading is maintained at this level. If repeated readings are less than 140/90 his blood pressure should be reassessed yearly.[10]
Case 17.3
| Possible diagnosis | Supporting factors in history |
|---|---|
| DDx 1: adhesive capsulitis | Diffuse shoulder pain, age of patient between 40 and 65, insidious onset, decreased range of motion (ROM), progressive nature of symptoms, unknown aetiology, history of diabetes |
| DDx 2: bursitis/tendonitis | Shoulder pain, pain worse at night, increased pain with activity, decreased ROM |
| DDx 3: rotator cuff tear | Shoulder pain, decreased ROM, pain worse at night, increased pain with activity |
| DDx 4: osteoarthritis | Diffuse shoulder pain, decreased ROM, age of patient |
| DDx 5: pancoast tumour | Severe, almost constant shoulder pain |
| DDx 6: referral from cervical spine | Possible, but less likely |
A relationship between diabetes mellitus and shoulder adhesive capsulitis has been shown in a number of studies. Balci, Balci, and Tuzuner found adhesive capsulitis in 29% of the type II diabetic patients that they studied.[11] The presence of diabetes in the adhesive capsulitis patient can signal the presence of other underlying complications.
| Examination | Justification |
|---|---|
| Active, passive, and resisted glenohumeral ROM | Differentiate between glenohumeral joint pathology and extra-articular derangements |
| Palpation | Determine specific location of pain, spasm, deformity |
| Yergason test | Evaluate biceps tendon |
| Apley test | Evaluate supraspinatus tendon, adhesive capsulitis |
| Dawburn sign | Evaluate for bursitis |
| Codman sign | Evaluate for rotator cuff weakness |
Shoulder examination should be performed bilaterally with the ‘good’ shoulder tested first.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


