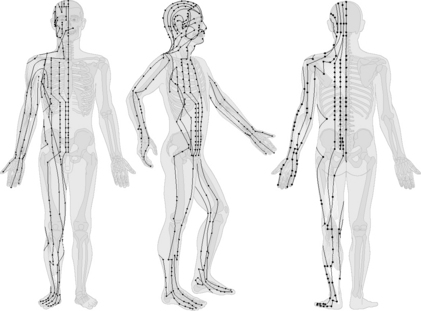
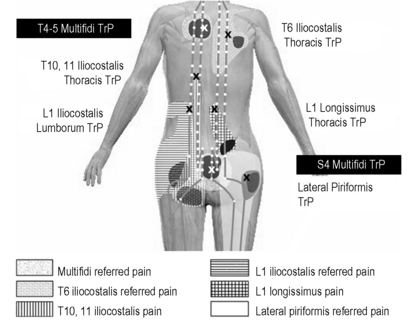
Chapter 7.9 Acupuncture as a fascia-oriented therapy Acupuncture has increasingly been used in Western medicine over the last three decades. It originated with traditional Chinese medicine (TCM) in the early Han period and has been described systematically for the first time in the medical compilation “Huangdi Neijing” (Yellow Emperor’s Inner Classic), whose texts date from the Han period (200 BCE to 200 CE) (Zhu 2001). Acupuncture means in its Chinese translation zhen jiu “needling burning”. However, before the development of steel needles, acupuncture consisted of skin irritation using sharp objects (e.g., stones), local warming at defined body sites, and minimal surgical interventions like blood letting. Nowadays, acupuncture is defined as needling at anatomically defined sites of the body (acupuncture points) or sensitive spots (ah shi points) for therapeutic purposes including so-called moxibustion, i.e., heating or warming of the skin at acupuncture points with the help of burning mugwort (Artemisia vulgaris) (Fig. 7.9.1). Fig. 7.9.1 • Choice of acupuncture instruments: different kinds of needles and of mugwort. From Irnich, 2008, with permission. All 360 classical acupuncture points lie strung together on the body surface according to a yin–yang pattern. They are arranged in three systems (front, back, and lateral aspects of the body). Qi is supposed to circulate within these meridians (Fig. 7.9.2). A remarkable observation to explain acupuncture points and meridians comes from myofascial referred pain that was observed to spread along the supposed meridian courses. Dorsher & Fleckenstein (2008a, 2008b) compared the anatomic correspondence of the “common” myofascial trigger point locations described in the Myofascial Trigger Point Manual to the locations of classical acupuncture points (Fig. 7.9.3). Anatomic correspondence of a common myofascial trigger point and a classical acupuncture point means those points are proximate and are demonstrated by acupuncture and anatomy references to enter the same muscle region. There is at least a 93.3% correspondence, if the distance between points on the skin is at most 3 cm; anyhow, points had to enter the same muscle region. At a maximum skin distance of 1 cm, 37% of points can still be found to correspond. There are marked clinical correspondences of both the pain indications (up to 97%) and somatovisceral indications (> 93%) of anatomically corresponding common myofascial trigger point–classical acupuncture point pairs (classical acupoints that are proximate to and enter the muscle region of their correlated common myofascial trigger points). The spread of deqi along the meridians seems to be the same phenomenon as the physiologically analogous concept of referred pain arising from myofascial trigger points in the myofascial pain tradition. This provides a clinical line of evidence that myofascial trigger points and acupuncture points likely might describe the same physiologic phenomena. Fig. 7.9.3 • Referred pain patterns of myofascial trigger points of the back and their correlation to the bladder meridian and its respective acupuncture points. From Irnich, 2008, with permission. These correlations make the explanation of the connecting meridians between acupuncture points more feasible. Speculation in this regard has continued since acupuncture’s earliest days as to whether acupuncture meridians are conceptual constructs or have an anatomic basis. Connective tissue might mediate acupuncture effects: Langevin (2002a) showed that rotation after needling activates fibroblast by mechanosensory transduction. These local effects can be tracked in distant connective tissue, too. Additionally, some researchers have described a degree of overlap of meridians and the peripheral nervous system in the extremities, whereas others have postulated that the meridians may exist in the myofascial layer of the body, reflecting perceived sensations by stimulating fascial structures. An interesting observation might be that anatomically derived myofascial meridians have distributions similar to those of acupuncture meridians described by TCM.
Introduction

Meridians
Physiologic background
Related posts:
 Deep fascia of the lower limbs
Scleroderma and related conditions
Interoception: A new correlate for intricate connections between fascial receptors, emotion, and self recognition
Diabetic foot
Membranous structures within the cranial bowl and intraspinal space
Fascia-related disorders: Hypermobility
Deep fascia of the lower limbs
Scleroderma and related conditions
Interoception: A new correlate for intricate connections between fascial receptors, emotion, and self recognition
Diabetic foot
Membranous structures within the cranial bowl and intraspinal space
Fascia-related disorders: Hypermobility
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Musculoskeletal Key
Fastest Musculoskeletal Insight Engine