Above-Elbow and Below-Elbow Amputations
Jacob Bickels
Yair Gortzak
Yehuda Kollender
Martin M. Malawer
BACKGROUND
Tumors of the upper extremity may cause extensive soft tissue and bone destruction and extend into the main neurovascular bundle. In those extreme situations, limb sparing may not be feasible, and amputation is required to achieve wide margins of resection and local tumor control.
Above-elbow amputations may be required for advanced soft tissue and bone sarcomas of the forearm and around the elbow (FIG 1A); below-elbow amputations are performed for such tumors of the forearm and the hand (FIG 1B).
Above- and below-elbow amputations are rarely done because the upper arm, elbow, and forearms are rare location for musculoskeletal tumors and because tumors at that site are noticed in relatively early stages and in most cases are resectable. Furthermore, administration of preoperative chemotherapy and availability of isolated limb perfusion have allowed to control the majority of patients that present with a large tumor.
Nonetheless, above- and below-elbow amputations retain a definitive role in the management of soft tissue and bone tumors of the upper extremity.
ANATOMIC CONSIDERATIONS
Above-elbow amputations can be metaphyseal (high), diaphyseal, or supracondylar (see FIG 1A).
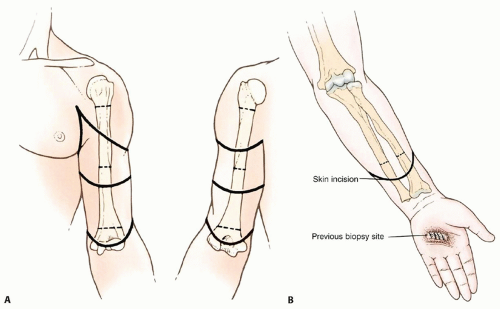
FIG 1 • A. Above-elbow amputations are done for advanced soft tissue and bone sarcomas of the forearm. Skin incisions and osteotomy sites for metaphyseal (high), diaphyseal, and supracondylar above-elbow amputations. B. Below-elbow amputations are done for advanced soft tissue and bone tumors of the forearm and hand. Skin incision and osteotomy site for below-elbow amputation.
High above-elbow amputations are those proximal to the deltoid tuberosity. Patients who undergo amputation proximal to the insertions of the deltoid and pectoralis major muscles have far greater difficulties adjusting to their prosthesis than do those who have undergone a more distal amputation.
Below-elbow amputations should preserve the maximal length of both radius and ulna. Although tumors of the hand are treated by a standard below-elbow amputation, performed through the distal third of the forearm, tumors of the distal forearm require a higher amputation and warrant special consideration. A minimum of 2.5 to 3 cm of bony stump, measured from the radial tuberosity, is required to preserve function. Additional length in a very short stump can be obtained by releasing the biceps tendon; adequate flexion of the stump will be provided by the brachialis muscle.
INDICATIONS
Extensive soft tissue and bone tumor extension with no option for reconstruction and reasonable function following resection (FIGS 2, 3 and 4)
Local recurrence was once considered a primary indication for amputation. The mere presence of a recurrent sarcoma is no longer an immediate indication for an amputation.
The capability to resect the recurrent tumor without compromising the function of the extremity is the determining factor on which the decision to amputate is based (FIG 5).

FIG 2 • A. Clinical picture and (B) plain radiograph showing metastatic carcinoma of lung to the mid-ulna with extensive bone destruction and soft tissue extension. C,D. Plain radiographs showing high-grade sarcoma of the proximal radius associated with extensive soft tissue extension. These tumors necessitate above-elbow amputation to achieve local tumor control and palliate pain.

FIG 3 • A. Clinical picture and (B) plain radiograph showing high-grade sarcoma of the first metacarpus. C. Fungating soft tissue sarcoma of the hand. D. Extensive necrotic and fungating sarcoma of the wrist. These tumors necessitate below-elbow amputation to achieve local tumor control.Related posts:
 Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
Dorsal Block Pinning of Proximal Interphalangeal Joint Fracture-Dislocations
Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
Dorsal Block Pinning of Proximal Interphalangeal Joint Fracture-Dislocations

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access
