PROCEDURE 9 Radial Head Fractures
Open Reduction and Internal Fixation
• The fracture must be amenable to anatomic joint reduction and rigid internal fixation. This will depend on:


Indications


 Associated longitudinal instability of the forearm (Fig. 3)
Associated longitudinal instability of the forearm (Fig. 3)• Fractures associated with longitudinal instability of the forearm (i.e., interosseous ligament injury)



Examination/Imaging
 Clinical evaluation
Clinical evaluation• The joint above and below the fracture should be examined for associated injury (e.g., associated distal radioulnar joint injury).
 Imaging
Imaging• Plain radiographs of the elbow in the anteroposterior (Fig. 4A) and lateral (Fig. 4B) planes must be obtained.
• A radiocapitellar view taken with the dorsal aspect of the supinated forearm against the x-ray plate with the beam directed 45° mediolaterally may help identify minimally displaced fractures of the radial head, coronoid, and capitellum.
• Radiographs of the ipsilateral and contralateral wrist should be obtained to determine ulnar variance if there is a question of longitudinal instability.
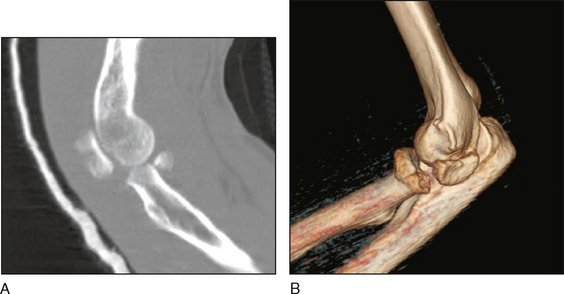
• Computed tomography scanning (Fig. 5A) with three-dimensional reformatting (Fig. 5B) allows better definition of the anatomy, the degree of comminution, and the size of the fracture fragments.

Surgical Anatomy
 Muscles and nerves
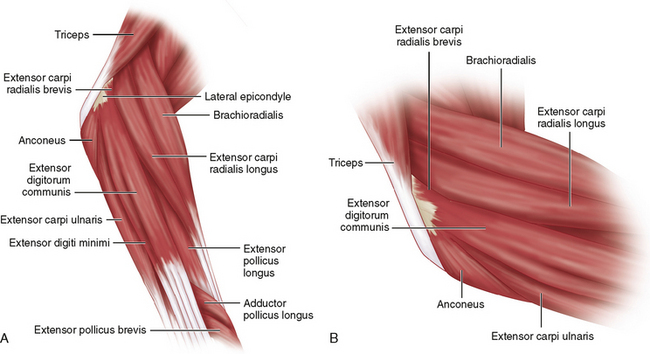
Muscles and nerves• Anconeus muscle/extensor carpi ulnaris (ECU) (Fig. 6A and 6B), as well as the extensor carpi radialis brevis (ECRB), extensor carpi radialis longus (ECRL), and extensor digitorum communis (EDC)
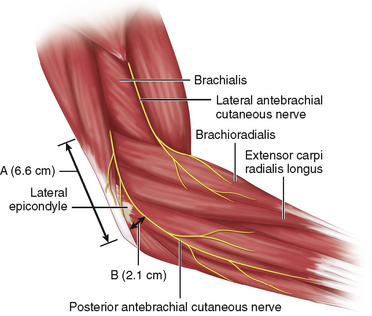
• Posterior antebrachial cutaneous nerve (PABCN; superficial and anterior to common extensor origin) (Fig. 7; LABCN = lateral antebrachial cutaneous nerve)

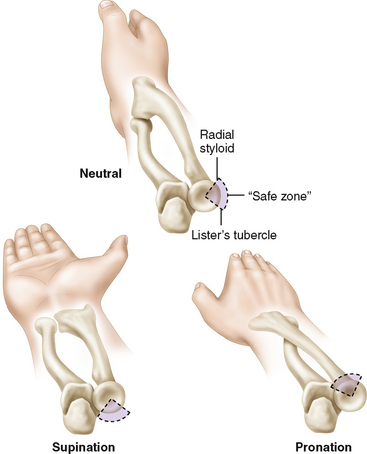
 The “safe zone”—100° arc of the circumference of the radial head that does not articulate with the radial notch of the proximal ulna (Fig. 11)
The “safe zone”—100° arc of the circumference of the radial head that does not articulate with the radial notch of the proximal ulna (Fig. 11)