This patient regularly has to remove her shoe while shopping. She is a 45-year-old research worker who presents with a sharp, shooting pain in the ball of her left foot and toes. The pain began as a burning, tingling sensation, which is now more intense and neuralgic in nature. She is only able to walk short distances. Relief of pain can be aided by massaging her foot or manipulating her toes. On examination, there is a sensory deficit in the region demonstrated in Figure 49.1. Pain is exacerbated by lateral compression of her forefoot (Fig. 49.2).
1 Name this condition and state the group of patients most commonly affected by it.
2 Which test is being carried out in Figure 49.2 and precisely where would you expect to localize pain?
3 Name additional investigations that are helpful in confirming a diagnosis.
4 Discuss the aetiology of this condition.
5 Outline a treatment plan for this patient.
 |
| Fig. 49.2 |

Morton’s neuroma
2 Using a thumb, firm pressure applied to the affected web space will elicit focal tenderness which may be exacerbated by simultaneously compressing the metatarsal heads together (see Fig. 49.2). This may be accompanied by a painful ‘Mulder’s click’. The third web space is most frequently involved, followed by the second. Symptoms never occur in either the first or fourth web spaces. The exact site of tenderness is located to a point between and just anterior to the heads of the two adjacent metatarsals. Other clinical signs and symptoms are summarized in Table 49.1.
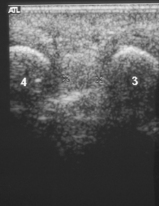
3 Ultrasonography is routinely used to detect neuroma. A typical sonographic appearance is that of a hypoechoic mass (varying in density from the surrounding tissue), orientated parallel to the long axis of the metatarsals (Fig. 49.3). Although the validity of ultrasound scans has been questioned, our approach is to confirm a swelling on the nerve with ultrasound before operation.
5 Conservative management starts with advice to the patient to change the style of their shoes. Broad, lace-up shoes are to be recommended and high-heeled, slip-on court shoes avoided. Insoles can only be considered if the footwear will accommodate them, or they will worsen the problem. Insoles such as metatarsal dome support will lift and spread the metatarsals. Orthoses can be used to reduce forefoot hypermobility.
An injection of corticosteroid is the third line of treatment. The evidence shows that this is effective but a recurrence of symptoms should be expected. If patients have a good response to an initial injection, then a second or even a third injection is possible but the risk of subcutaneous fat atrophy and hypopigmentation increases (see Fig. 49.4). There is only limited evidence for the use of alcohol injections. Beyond this, surgery has to be considered (Fig. 49.5). A dorsal incision is probably preferable as it avoids the risk of a troublesome scar and also allows early postoperative weightbearing.
A four-stage treatment plan is summarized in Figure 49.6.
 |
| Fig. 49.6 |
Injection of corticosteroid is a standard treatment for Morton’s neuroma.
| Solution/volume | Methyl prednisolone 0.5 ml (20 mg) and lignocaine hydrochloride 1 ml (2%) |
| Needle | A 25 gauge (blue) or 27 gauge (long) needle is ideal |
| Technique of injection | Locate the painful intermetatarsal space, invariably the second or third. Identify the metatarsal heads and, from the dorsum, introduce the needle just proximal to the level of the metatarsal heads. Penetrate until resistance of the plantar skin is met. Withdraw the needle about 0.5 cm, aspirating to avoid intravascular injection, and then inject half the volume of contents of the syringe. Withdraw the needle a further 0.5 cm and inject the remainder |
A systematic Cochrane review concluded that there is insufficient evidence with which to assess the effectiveness of surgical and non-surgical interventions for Morton’s neuroma. Subsequently one randomized controlled trial of 125 patients has demonstrated that a single injection under ultrasound guidance is effective in the treatment of this condition at 3 months, but that this is not of long-standing benefit. Concurrently an economic analysis showed that this treatment may not be cost effective. The literature suggests a success rate of 70–80% for surgical excision of the nerve.
| Subjective symptoms | Objective symptoms |
|---|---|
• Sharp, lancing or cramp-like pain often likened to a burning hot needle • Pain only on walking • Patient has to stop walking • Patient has to rest until pain goes (relief aided by removing shoes and massaging toes) • Pins and needles or numbness experienced between toes | • Pain located in second or third web space elicited with plantar pressure and exacerbated by lateral compression • Painful Mulder’s click present • Loss of sharp sensation between toes • Injection of local anaesthetic temporarily ameliorates pain |


Key points
• Morton’s neuroma is common, occurring mainly in the third web space.
• Pain is characteristically paroxysmal and limits walking.
• Footwear is the dominant causative factor.
• Management is directed at advice on footwear, use of insoles and corticosteroid injections.
• Excision of the nerve remains the mainstay of treatment.
Further reading
Fanucci, E; Masala, S; Fabiano, S; et al., Treatment of intermetatarsal Morton’s neuroma with alcohol injection under US guide: 10 month follow-up, European Radiology 14 (3) (2004) 514–518;
Hassouna, H; Dingh, D; Taylor, H; Johnson, S, Ultrasound guided steroid injection in the treatment of interdigital neuralgia, Acta Orthopaedica Belgica 73 (2) (2007) 224–229.
Hughes, RJ; Ali, K; Jones, H; Kendall, S; Connell, DA, Treatment of Morton’s neuroma with alcohol injection under sonographic guidance: follow-up of 101 cases, Am J Roentgenol 188 (6) (2007) 1535–1539.
Sharp, RJ; Wade, CM; Hennessy, MS; Saxby, TS, The role of MRI and ultrasound imaging in Morton’s neuroma and the effect of size of lesion on symptoms, Journal of Bone and Joint Surgery 85 (7) (2003) 999–1005.
Thomson, CE; Martin, D; Gibson, JNA, Treatment interventions for Morton’s neuroma: a systematic review. Cochrane Database of Systematic Reviews. (2004) ; Issue 3.
Thomson, CE; Beggs, I; Martin, D; et al., Focus on Research. Steroid injections (methylprednisolone) in the treatment of Morton’s neuroma: patient-blind randomised trial. Scottish Executive Health Department, Chief Scientist’s Office. (2007) ; Available online at www.sehd.scot.nhs.uk:80/cso/index.htm.
Case 50
This single 25-year-old man would like to wear a kilt! Unfortunately he is extremely self conscious about the appearance of his leg (Fig. 50.1), supposedly injured as a young child when he fell off the back of a motorcycle whilst growing up in India. There was no evidence of any proximal injury. On further questioning, he is aware that as a child he had been quite ill with a fever. Functionally, he has a 5 cm limb length discrepancy although he walks reasonably well despite a flail right foot. He has been helped with surgery in childhood (Fig. 50.2) but he has a residual calcaneus deformity. On the right side he weight bears only on his heel (note the hypertrophy of the heel pad; Fig. 50.3). He is now living in the UK and seeks help with the cosmetic appearance of his right leg.
2 Which clinical investigations are required to confirm this diagnosis?
3 Which operations have been performed on his right foot?
4 What conservative measures could be offered to help this young man?
 |
| Fig. 50.1 |
 |
| Fig. 50.2 |
 |
| Fig. 50.3 |
Poliomyelitis
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


