4 The Shoulder
4.1 Arthroscopic Synovectomy of the Shoulder Joint
Indication
Therapy-resistant Larsen 0–II/III synovitis after optimization of medication therapy and cortisone injections. Significant clinical symptoms and loss of mobility.
Specific disclosures for patient consent
Recurrence. Infection. Radiosynoviorthesis (and/or chemosynoviorthesis) may be necessary 6 weeks postoperatively.
Instruments
Standard shoulder arthroscope. Special items: shaver system. Electrocautery.
Position
Beach chair position with arm freely mobile (Fig. 4‑1 ).
Approach
Specifics
Preoperative ultrasound is used for evaluation of the major extra-articular bursae; these may necessitate an open procedure. Mark the anatomical landmarks (acromion, coracoid, scapular border, clavicle) after sterile draping and prior to making an incision.
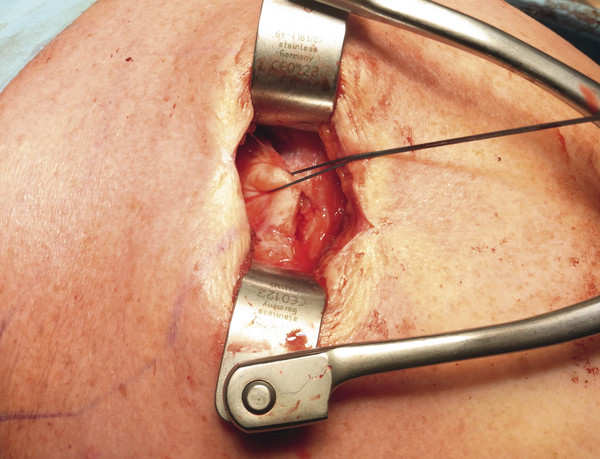
Surgical technique
See Fig. 4‑4, Fig. 4‑5, Fig. 4‑6, Fig. 4‑7, Fig. 4‑8, Fig. 4‑9.









4.2 Rotator Cuff Tear
Indication
Larsen I–II destruction. Rotator cuff tear diagnosed by radiographic imaging (MRI scan, ultrasound).
Operatively reconstructible rotator cuff tear: based on size on MRI scan and no evidence of fatty degeneration of musculature on MRI scan. Acromiohumeral interval greater than 6 mm.
If there is any uncertainty, rotator cuff mobility can be examined arthroscopically.
Specific disclosures for patient consent
Failure of tendon integration. Re-rupture (also secondarily with cranialization of the humeral head). Shoulder stiffness. Injury to blood vessels, nerves (for example, axillary nerve).
Instruments
Standard shoulder arthroscopy pan. Shoulder pan. Anchoring system from the manufacturer of choice.
Position
Beach chair position (Fig. 4‑10 ).
Key steps
Proceed in the same fashion as for shoulder arthroscopy. Every rheumatoid shoulder first undergoes arthroscopy, see Chapter 4.1.
Synovectomy is initially performed arthroscopically on each patient. The inflamed bursa is removed during the subsequent subacromial arthroscopy. Rotator cuff mobility is assessed. Small ruptures are closed arthroscopically, although these are relatively uncommon in rheumatoid patients. The quality of the rotator cuff tissue surrounding the rupture is frequently poor and is usually associated with severe subacromial inflammatory changes. As a result, a mini-open approach is often chosen.
Surgical technique
See Fig. 4‑11, Fig. 4‑12, Fig. 4‑13, Fig. 4‑14, Fig. 4‑15, Fig. 4‑16, Fig. 4‑17, Fig. 4‑18.
Postoperative aftercare
Immediate full-range mobilization (caveat: no shoulder immobilization). For large ruptures, use a shoulder abduction pillow for 6 weeks.








Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


