PROCEDURE 29 Proximal Tibia Fractures: Intramedullary Nailing











Surgical Anatomy
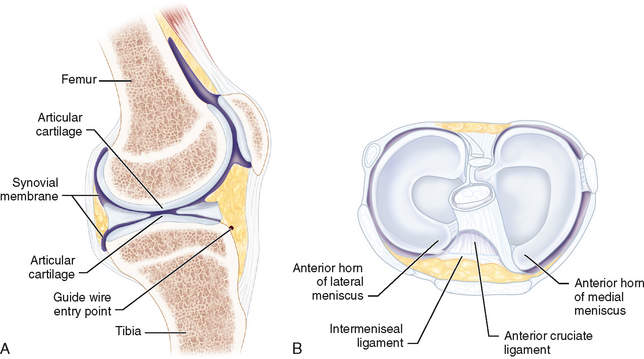
 The entry point in the proximal tibia (Fig. 2A) can endanger the menisci, intermeniscal ligament, and articular surface (Fig. 2B).
The entry point in the proximal tibia (Fig. 2A) can endanger the menisci, intermeniscal ligament, and articular surface (Fig. 2B).
Positioning

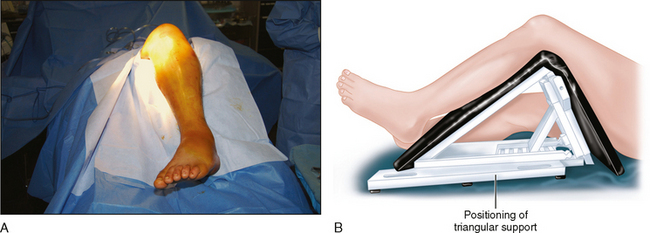
 An adjustable triangular frame is used to support the limb (Fig. 3A and 3B). This allows the knee to be supported in variable degrees of flexion during the procedure.
An adjustable triangular frame is used to support the limb (Fig. 3A and 3B). This allows the knee to be supported in variable degrees of flexion during the procedure.