PROCEDURE 12 Open Reduction and Internal Fixation of Forearm Fractures
Indications
• Distal radioulnar joint (DRUJ) instability is associated with the location of the radial shaft fracture: 55% of isolated radial shaft fractures located within 7.5 cm from the midarticular surface of the radius were associated with DRUJ instability, whereas only 6% of fractures located beyond 7.5 cm from the midarticular surface of the radius were associated with DRUJ instability.





Examination/Imaging



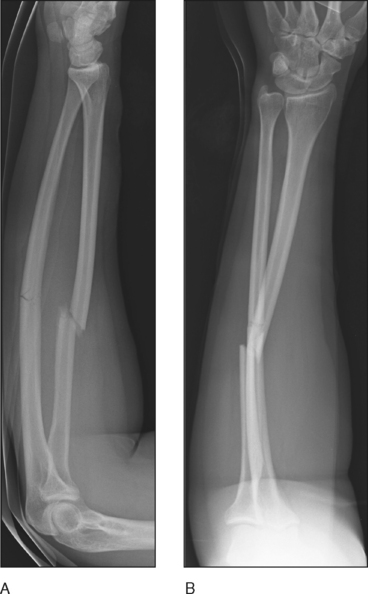
 Anteroposterior (AP) and lateral radiographs of the forearm. Figure 1 shows orthogonal radiographs of combined radial and ulnar shaft fractures.
Anteroposterior (AP) and lateral radiographs of the forearm. Figure 1 shows orthogonal radiographs of combined radial and ulnar shaft fractures.
Surgical Anatomy
• Closed reduction with long-arm cast immobilization is reserved for pediatric fractures and isolated fractures of the distal two thirds of the ulnar shaft.
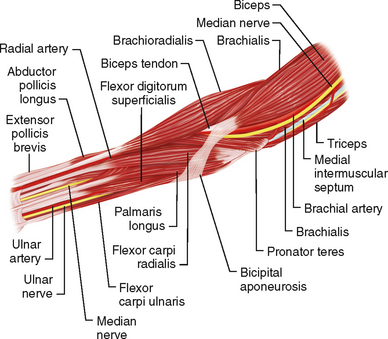
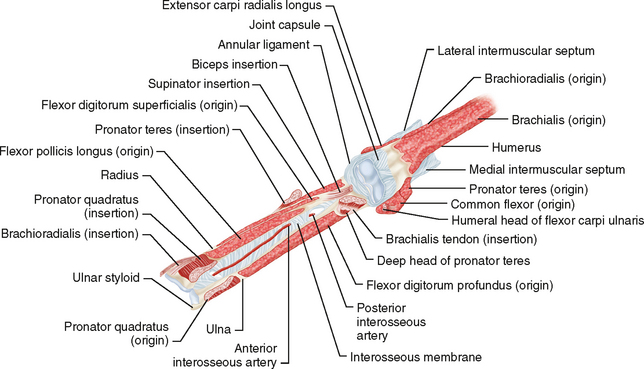
 Volar anatomy of the radius
Volar anatomy of the radius• Superficial layer: brachioradialis muscle, flexor carpi radialis muscle, superficial branch of the radial nerve, radial artery
♦ Figure 2 shows the superficial layer of the volar forearm; note the interval between the brachioradialis (radial side) and the pronator teres/flexor carpi radialis (ulnar side).
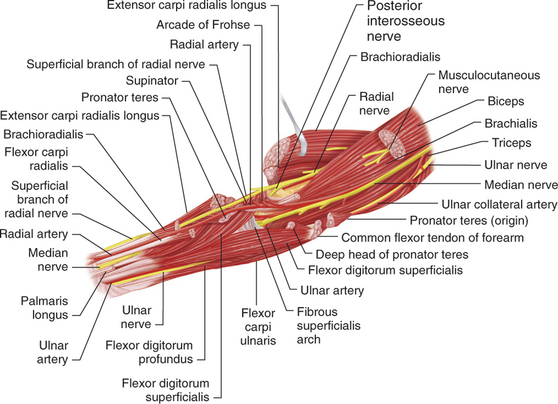
• Deep layer
♦ Figure 4 shows the deep layer of the volar forearm. Note the insertion of the pronator quadratus on the distal third, the flexor pollicis longus and flexor digitorum superficialis on the middle third, and the pronator teres and supinator on the proximal third of the radius.
♦ Middle third of radius: pronator teres muscle, flexor pollicis longus muscle, flexor digitorum superficialis muscle (see Fig. 4)

Positioning
 The patient is placed supine on the operating table with the affected arm placed on an armboard. The forearm may be supinated to allow for a volar approach to the radius, or pronated to allow for an approach to the ulna.
The patient is placed supine on the operating table with the affected arm placed on an armboard. The forearm may be supinated to allow for a volar approach to the radius, or pronated to allow for an approach to the ulna.





