Review of Musculoskeletal Radiology
Emory University School of Medicine, Atlanta, GA, USA
Introduction
Imaging in the rheumatic diseases is often a key component of diagnosis and management. This section will review classic radiographic features of rheumatoid arthritis, psoriatic arthritis, crystalline arthropathies, and other syndromes commonly seen in the field of rheumatology.
Radiographic Features of RA
- Symmetric and polyarticular joint involvement
- Predilection for hands (MCP, PIP), wrists, and feet (MTP), but elbows, knees, shoulders, and hips also can be affected in aggressive or longstanding disease
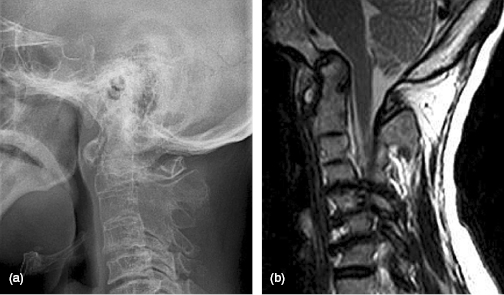
- Cervical spine involvement also occurs including facet erosions, cranial settling, and C1–C2 subluxation
- Early manifestations (Figure 11.1)
- Periarticular soft tissue swelling
- Periarticular osteopenia
- Marginal erosions – begin at “bare areas” – intercapsular articular margins, usually at the ulnar styloid, MCP 2 and 3, and the fifth MTP before other areas are affected
- Periarticular soft tissue swelling
- Late manifestations (Figures 11.2, 11.3)
- Diffuse osteopenia
- Joint space narrowing
- Erosions at both proximal and distal phalanges
- Ulnar deviation
- Joint subluxation and dislocation with characteristic deformities
- Swan-neck deformity – hyperextension at PIP and flexion at DIP
- Boutonniere deformity – flexion at PIP and hyperextension at DIP
- Windswept deformity – symmetric ulnar subluxations and dislocations of the MCP and PIP joints
- Hitchhiker’s thumb: flexion of MCP and hyperextension at IP joint
- Ankylosis (fusion) of joints – most often carpals and tarsals
- Secondary osteoarthritic changes: osteophyte formation, subchondral sclerosis, subchondral cyst
- Erosions at both proximal and distal phalanges
- Diffuse osteopenia



See Figures 11.4, 11.5.
Radiographic Features of Psoriatic Arthritis
- Polyarticular inflammatory arthritis affecting primarily the joints of the hands and feet
- Bone density is normal
- DIP involvement is common; wrist involvement is rare
- Joint involvement is typically asymmetric
- Early erosive changes progress to severe subchondral erosions, primarily at proximal phalanges of involved joints (Figure 11.6)
- Enthesophytes can be seen at sites of enthesopathy (Figure 11.7)
- Soft tissue swelling may involve the entire digit, termed a “sausage digit” or dactylitis
- Productive change or periostitis occurs at distal articular surfaces of involved joints as well as along the length of involved phalanges
- Advanced disease can produce a classic “pencil in cup” deformity with erosion of the proximal phalanx into a “pencil,” and productive changes along the distal periarticular surface into a “cup” (Figure 11.8)
- Arthropathy may precede the development of psoriasis in up to 20% of patients
- Figure 11.9 illustrates telescoping digits and arthritis mutilans. See also Table 11.1




| Psoriatic arthritis | Rheumatoid arthritis | |
|---|---|---|
| Symmetric joint involvement | No | Yes |
| Juxta-articular osteopenia | No | Yes |
| DIP involvement | Yes | No |
| Wrist involvement | Rare | Common |
| Dactylitis | Yes | No |
| Periostitis | Yes | No |
| Enthesophytes | Yes | No |
| Subchondral cysts | Rare | Common |
Table 11.1 Distinguishing psoriatic arthritis from rheumatoid arthritis.
Radiographic Features of Ankylosing Spondylitis
- Mixed erosive and productive arthritis
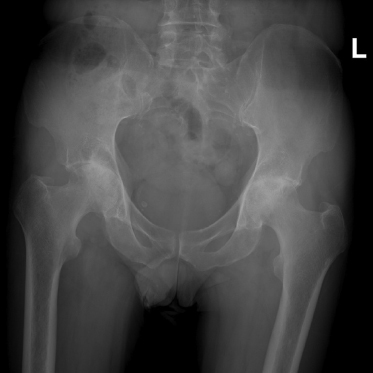
- Involves primarily the axial skeleton and may involve the large proximal joints
- Sacroiliac joint involvement is a hallmark of the disease, more prominently on the inferior, iliac side of the joint (the synovial portion) in early disease but later involving the entire joint
- The superior pole of the sacroiliac joint is made primarily of ligaments that can form bridging enthesophytes
- Bridging enthesophytes can also be seen in:
- DISH
- Chronic reactive arthritis
- Psoriatic arthritis
- Vitamin D toxicity
- Disease progression leads to sacroiliac joint fusion and subsequent progression cranially to involve the thoracolumbar spine
- Vertebral involvement begins at the peripheral corners of the vertebral body, where enthesitis and reactive sclerosis induces the “shiny corner” sign
- Subsequent erosion at the peripheral corners of vertebral bodies induces loss of normal concavity, leading to a squared appearance of vertebral bodies on lateral films (Figure 11.10)
- Further progression of the disease in the thoracolumbar spine includes ossificiation of the annulus fibrosis, or syndesmophytes
- End stages of ankylosing spondylitis show ankylosis or fusion of the vertebral bodies into the classic finding of “bamboo spine” (Figure 11.11)
- Figure 11.14 illustrates the complications of ankylosing spondylitis
- Sacroiliac joint involvement is a hallmark of the disease, more prominently on the inferior, iliac side of the joint (the synovial portion) in early disease but later involving the entire joint








