CHAPTER 10. Practical bodywork in labour
Refer to labour theory (Chapter 2 and Chapter 13)
For more information on:
What happens during labour
Different types of medical interventions
Introduction
Bodywork during labour is quite unlike bodywork at any other time. The therapist does not know when or for how long they will need to be working with the client. It could be for a few hours or over the course of several days. It can be anytime within a month- long period (from 2 weeks before the due date and up to 2 weeks after) and during this time the therapist needs to be in relative proximity to the client. This means curtailing travel, late nights, loss of sleep and abstaining from partying or consuming alcoholic beverages. Being available 24 hours a day in this capacity involves making a substantial commitment to the woman/family having a baby.
In some respects professional boundaries become different at this intimate stage in a client’s life. Work may need to be done while the client is experiencing nausea and vomiting, while she is on the toilet, or in situations where her realities of privacy and nudity are quite different from the clients seen in regular practice.
It is also essential that the therapist is able to communicate and work with the client’s partner, who may or may not be the father of the baby. Partners may be unsure and frightened and just as much in need of support as the woman. Work may need to be done with both to provide the best care possible. If there is no partner, the therapist may be the only support person apart from the primary care providers. In all situations, body work needs to be appropriate to the environment and relevant to the tasks of all others attending the birth.
Once the baby is born, it may need to be held, especially if the woman needs medical attention such as suturing. Appropriately qualified therapists may provide bodywork for the baby.
Much of the therapist’s role during labour may not be bodywork in the traditional sense. It may be that all that is done is to apply pressure to the sacrum or hold the woman’s hands for minutes or hours. It may be that as much time is spent wiping the woman’s face with a cool cloth, giving emotional reassurance, or helping her to get into supporting positions for labour as actually applying bodywork skills. Knowing what to do, when – and when to do nothing – is essential.
The work may be provided in the client’s home, or in the hospital – different environments in which to work and each with particular considerations.
It may be a time full of challenges, not only because it is not possible to plan in advance and is a process of continually responding to the unknown, but also because the length of labour may bring physical challenges to therapists as well as our clients. The therapist may become exhausted. Like the woman and partner in labour, the therapist must look after him- or herself, eating and resting where possible. This is both a personal responsibility and a responsibility to other clients.
Some therapists may decide that they do not want to take on the unpredictable and emotionally heightened opportunity of providing labour support. If the therapist has a young family or a complex schedule which can accommodate few alterations, it may simply not be practical to be out in the middle of the night or to drop everything at a moment’s notice. It may be preferable to teach some useful bodywork techniques to the partner at an organised birth preparation session in the weeks leading up to the birth, or agree to be accessible for phone support, or to even drop by, if timing allows, to provide an hour or two of support without attending the birth in its entirety. Other therapists may enjoy birthing support work so much that they seize every opportunity to be present at this amazing moment in a woman’s life and the life of the new baby. It truly teaches us a lot about the power, resilience and strength of the female body.
However, in deciding to work with women in labour, either helping them preparing before or by physically being at the birth, the therapist needs to be thoroughly familiar with the physiology of labour, including the different stages, and how to support the woman not only with bodywork, but also with positioning and breathing/visualisation. The therapist also needs to be aware of how to give appropriate emotional support. The power of the mind is as important as the power of the body during labour. Knowledge of types of medical intervention at different stages and their effects, as well as knowing the kind of bodywork which may or may not be appropriate if such interventions occur, is important.
In a sense, working with a woman in labour is one of the easiest times to do bodywork. A woman in labour is extremely sensitive to the kind of touch she needs and where she needs it. It is simply a matter of observing, watching the client’s body language, and listening to her. However, it is important to be adaptable. One woman may want to be touched a lot, another not at all. The main difference between labour work and ‘normal’ bodywork is that often the woman simply wants to be held: held in a particular area, held on a particular point. The woman may have very different needs at different times during labour or she may want the same kind of support throughout. The only thing that can be said with certainty about labour is that it is unpredictable. No two labours are the same.
It is important to remember labour could be 1 hour long or more than 30 hours long. It could be painful or pain-free. Essentially labour support is about accompanying the woman in a journey into the unknown. While the therapist is present, he or she needs to be able to stay with the process of that journey as it unfolds.
This kind of approach was often a form of traditional labour support. The birth partner would often be a wise woman in the village, experienced in giving emotional and physical support. It is a pity that some aspects of this approach are missing from much current intrapartum care. Modern medical care is indispensable and potentially life saving when things go wrong but is not as well developed in supporting the natural processes of women’s bodies. Rather than ensuring women’s bodies function at their best during birth, it has achieved some of its benefits at the cost of causing women to have less trust in their own inner resources. Body processes sometimes do go awry. In this regard women today are luckier than their ancestors – they can turn to drugs and medical interventions if they are needed. However, currently drugs and interventions are often seen as the first way to approach birth, not the last.
What has to be remembered, which is often forgotten, is that birth is essentially a natural process and one that women’s bodies are designed to be able to cope with, even in this technological age. In many cultures, birth was considered a spiritual process, a gateway between adulthood and womanhood, a key life transition. In modern cultures, where the emphasis tends to be on controlling many things, including our bodies, the simplicity, power and miraculousness of birth has been forgotten. One of the aspects of the therapist’s role is to support this amazing process as much as possible.
For woman and partner
Offers tools to support the woman to:
• Be more aware of her baby.
• Trust in birth and increase her confidence that she can have a positive birth experience.
• Examine her attitudes, needs and hopes for her birthing experience.
• Provide strategies for working with pain.
• Include her partner by offering practical strategies for them to be involved during labour.
For baby
• May help the baby get in good position for labour (optimal fetal position).
• If the woman is more relaxed it will tend to create a more relaxing environment for the baby.
• Helps support prenatal bonding between the parents and their baby.
Other potential benefits
• Shorter labour, decreased need for caesarean deliveries, forceps, vacuum extraction, oxytocin augmentation and analgesia.
• Less difficult and less painful labour.
• Reduction in anxiety scores, positive feelings about the birth experience, increased rates of breastfeeding initiation.
Postpartum benefits
These include decreased symptoms of depression, improved self-esteem, exclusive breastfeeding, and sensitivity of the woman to her child’s needs.
10.1. Overview of practical labour work themes
Supporting the physiological process of labour
As a bodyworker, a prime aim is to support the woman in whatever choice she makes in relation to her pregnancy and her birth. However, a key aspect of birth work is knowing how best to support the physiological process. This will include knowing which positions and movements best support this process, and what type of bodywork is likely to be most effective. The birthing positions utilised by the client will affect the type of work which is possible. For example, if the client is leaning forward, the therapist may need to be physically supporting her, which will limit the possibilities for hands-on work. If the woman is leaning forward in a pool, then the therapist may be unable to reach her back.
Working if medical intervention becomes necessary
Even if the client needs medical interventions it is often possible to continue to support her. Depending on when, why and how an intervention is chosen, the woman may be experiencing stress and/or pain and she will still need support. It is necessary to know how to change the focus of work. It is possible to enable a woman to maintain elements of her preferred birthing strategies in the face of medical decision making. For example, although the woman may be monitored throughout her birth, the therapist may be able to help her remain in an upright position. If a caesarean section becomes necessary, then the woman may want some support, regardless of whether the therapist is allowed into the actual delivery room. This may include giving emotional and/or physical support both immediately prior to and as soon as possible after the surgery.
Working with the breath
Breathing well is a fundamental part of labouring well. It ensures both woman and baby get an adequate supply of oxygen. The woman is more likely to stay calm and relaxed, thus increasing the hormones of oxytocin and endorphins which help her during labour. As the woman and baby are so connected this may have a positive effect on the baby too.
Childbirth classes in the 1970s tended to emphasise techniques of ‘psychoprophylactic breathing’, which are primarily dissociation techniques. These use breathing methods which try to get the woman to disconnect from pain in her body and focus on something outside. However, the current emphasis in childbirth education courses is to emphasise simple techniques which focus on connecting to the body. These tend to utilise a slow, deep relaxed pattern of breathing, often focusing on the out-breath. Prior to the birth, the therapist can help the woman explore what works best for her and if present during labour continue to support the woman to be able to focus on finding the most effective rhythm of breathing. It may be supportive to breathe with her. Using pressure and holding techniques alongside breath awareness can be additionally effective. If the woman prefers to focus on something outside her body – a technique, an image, a movement – the therapist needs to be able to support her to do so.
Working with contractions
Women usually find that they manage better if they focus on one contraction at a time – one contraction is not so overwhelming to successfully cope with. The therapist can support and encourage this.
In a labour which starts naturally (i.e. not induced), the contractions often start by being weaker in intensity, although some women experience intense contractions early on in labour. Some women are very aware of the uterus/abdomen tightening and it may or may not be painful to them. Some women feel pain from the contractions referred down into their back or their legs. Most women find it best to accept and work with the feelings of each contraction.
Contractions are often experienced as wave-like – building up in the body to reach a peak of intensity and then fading away gradually, so that the woman has time to get used to each contraction before it reaches its most intense moment. It is usually helpful to use comfort strategies as the contraction is beginning, so that the peak of it does not take the woman by surprise. Highly important is that for most women there is some space between the contractions which need to be used for rest, recovery, and to prepare for the next contraction. This will help to prevent exhaustion and conserve energy for both the woman and her support person.
An induced labour tends to be more intense, depending on how it is facilitated and how the medication is administered. With induction via oxytocin, the contractions are less like waves and have a more constant intensity, so that there is not the same kind of build up at the peak of a contraction, nor the rest in between. Some women can cope with these contractions without the need for medical pain relief, but they may require more focus to cope with them effectively.
As labour progresses, many women begin to find their own rhythm. This may suggest a dance-like activity with its creative, repetitive, appearance.
Some women find that focusing on something outside themselves such as an external object or a word or phrase may help block pain out (dissociation). However, many women find it is more helpful to use something related to what the contraction is doing (association). This could be a mental image such as a cresting wave or climbing and descending a mountain in the first stage, or a bulb pushing through the ground for the second stage. It is important to spend some time exploring with the client in advance what images she thinks are likely to work best for her if possible.
Some women find that certain bodywork techniques help the contraction to be less painful, or less frightening, and they allow them to relate to it in a positive way.
Many women can keep an intense focus for at least 24 hours but after this they tend to get more tired, especially if they have not been able to rest or eat much. However, women can focus for a lot longer. Some women keep going for 30 or 40 hours or more. If the woman is prepared well, has good support and keeps her focus it is amazing what inner strengths she may find to draw upon. Bodywork is a powerful tool for supporting this process.
Working with ‘pain’
Many people argue that defining what happens during the birthing process as ‘pain’ immediately sets up certain expectations. Birth is certainly intense but its sensations may be unlike what is normally associated with ‘pain’. Pain usually indicates that something is wrong with the body, whereas for the most part, birth is about the body doing what it is designed to do. Of course sometimes the body runs into difficulty; the baby may not descend, is positioned awkwardly, or the uterus becomes fatigued, and this can create sensations of pain.
Rather than feeling pain, some women feel intense sensations. Many childbirth methods emphasise seeing contractions as ‘rushes’, thanks to the excellent midwifery work of Ina May Gaskin and the midwives of The Farm in Tennessee (Gaskin 2002). Others call them ‘surges’ rather than ‘pain’ (hypnobirthing term). This certainly gives a more positive focus to birth. However, most women do experience pain or at least discomfort during labour and it is worth being prepared for that reality. In terms of bodywork for pain relief, if the woman is supported to be as relaxed as possible, she tends to feel less pain or is able to cope with it better.
Both traditionally and even today in Japan, where shiatsu originates, women were just expected to get on with labour and, not surprisingly, with that expectation, they often do. The aim of bodywork is not necessarily to take away all pain. Sometimes pain serves a purpose, for example in making the woman aware that she needs to change position to get more comfortable. The ultimate aim is to enable the woman to work with her body, whatever happens. Working with a woman during pregnancy helps prepare for this.
Working with an awareness of the baby and fetal position
Working with an awareness not only of the woman, but also of the baby is important. After all, it is an unknown journey for the baby as much as the woman. Often for the woman, focusing on her baby, rather than on pain, gives a more positive perspective.
The position that the baby is in at the start of labour will have an effect on the outcome of birth.
It cannot be known with any certainty how much the baby is emotionally aware of the process of labour, but certainly it is actively engaged with the process. Babies have been shown to release oxytocin in the womb and therefore may contribute to initiating the process of labour (Odent 2001, Hitchcok 1980). As the baby progresses down the birth canal it is getting into the optimal position for birth, and it is the pressure of the head on the perineum which releases the prostaglandins, which in turn stimulate the production of more maternal oxytocin to strengthen expulsive contractions.
It makes sense for both therapist and woman to be aware of what is happening for the baby and to try to support it, either through including it with touch or through talking to it.
Working with involvement of the partner
Introducing the partner to bodywork for labour during the last trimester is helpful, whether or not the bodyworker has been invited to be at the birth. If the bodyworker will not be present then the role is to identify with the couple what they want to learn. What can be taught will depend on what the partner wants to use as well as their prior knowledge. They could be taught shiatsu labour focus points and other aspects of labour support. The most important aspect is to teach them to work with feedback from the woman so that if it does not feel right, then they alter or discontinue the technique until they have rechecked with the therapist.
If the therapist is going to be present, often the woman’s partner will also be present. It is vital to establish the role of the bodyworker/doula and the role of the partner as much as possible prior to labour. It may be that the partner wants to give emotional support while the therapist is there to give the hands-on support. However, the partner may be interested in learning bodywork skills in order to work alongside the therapist.
Working with awareness of the importance of the birth environment
The type of environment will affect the process of labour. Most therapists try their best to create a lovely space in which to give treatments. Similar aesthetic and supportive environments can be created during labour if possible. For those therapists working in hospital settings or places where there is little control of the surroundings, it is still worthwhile being aware of the setting and how best to encourage the creation of a supportive environment. It is worth talking to the woman before labour about how she can create the kind of space she wants, whether she is at home or in hospital.
I was once working with a family in the hospital setting. The lights were dim, my client was comfortably positioned in semi-reclining, and we were doing a repetitive, soothing massage. The nurse came vibrantly through the door and then instantly slowed her movements and tone of voice down to match the setting in the room. Later she told me she felt like a Tasmanian Devil – the hectic pace in the unit outside led to a level of frantic activity which was in direct contrast to the peace within our birthing room.
(Cindy)
Supporting a woman at home
This may be the easiest place to support the woman as she is in her own familiar environment. She has the benefit of knowing her own space, using her own possessions, and can do exactly what she wants. If the birth is going to be at home, then communication with the midwife and support people is needed to let them know the state of her labour when it begins.
If the woman is going to give birth in the hospital, she needs to know at what point her care provider wishes her to travel to the hospital.
Positions which support the physiological process of labour
If the woman is aiming for a natural birth, then the therapist will be working with the woman in positions which support the physiological process of labour.
These are:
• Upright, forward and leaning.
• Using gravity.
• Allowing the sacrum to move.
Common positions are:
• Standing: rocking, leaning against something.
• Squatting: full squat, supported squat or standing squat.
• Forward leaning: for example over a ball.
• Forward sitting.
• Lateral.
The basic positions are the same for the first and second stage of labour, and to some extent the third stage, to facilitate the delivery of the placenta. The main differences are that during the first stage of labour the emphasis is on relaxation and opening up the pelvis. In the second stage the emphasis is more on bearing down with a little more effort and focus.
These tend to be the same positions which women find comfortable at the end of their pregnancy, particularly the forward leaning positions (Fig. 10.1). The main difference in labour, however, is that the woman is likely to be moving around. The woman will need to practise these positions in the weeks leading up to labour and the therapist can support her to do this. The role of the therapist or support person during labour is often to offer suggestions regarding positioning, to help support her in these positions, and to help her change positions when desired. Resting versions of each position need to be encouraged so that the woman can rest as much as possible during labour, particularly during the quiet space between contractions. If any position appears to be slowing down labour, or labour is not progressing, it is often wise to suggest a change of position.
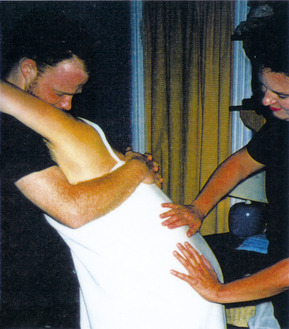 |
| Fig. 10.1 Birth: direct hands-on technique. |
If the woman needs to have some medical intervention then she may be placed in a position which is more convenient for the care provider. However, if the woman is uncomfortable, the therapist may be able to help the woman negotiate alterations for comfort. The therapist may also need to remind both the woman and caregiver to aware of PGI/SPD issues.
Supporting a woman to labour in water
The birth positions are essentially the same, except of course the woman cannot rest with her head lower than her hips. Water is especially good if the woman has pelvic girdle instability issues, provided she can get in and out of the pool in such a way that she does not aggravate the problem.
The therapist should not get into the pool with the woman for reasons of health and safety (blood and other body fluids and risk of infection). This means that most of the work is done with the neck and the shoulder and arms, and perhaps the back, if reachable. If the partner is in the pool with the woman s/he can be encouraged to do the work on the abdomen and sacrum.
The woman may use this for first stage or she may decide to stay in to give birth in the water. Midwives who have experience delivering babies in water should be sought for the client’s primary care if the woman wants to consider this as an option.
Testimonial of birth support
S.H., birthing client/RMT, doula, Canada
Having spent 2 years at massage school and having learned the benefits of massage during labour, it felt natural that we would have a massage therapist friend attend the birth of our first child. I called her to come to our home when we realised that ‘this was it’ and after a brief adjustment to a new Energy in our midst, I relaxed into her repetitive strokes. It was the first birth for my friend and although a bit nervous she was very happy to be told (at times in no uncertain terms!) what felt good and what did not. As she had no previous birth support experience, it was necessary for me to offer direction vs her responding intuitively to my needs. It was the pressure on the sacrum that really worked for me, with the strokes matching rhythm with the contractions. It took a bit of experimentation to figure out what felt best but once there I would not let her hands leave my back; in fact I was amused to find after it all that my low back was raw from so much rubbing. And so, I had my team – the RMT gave some physical relief of rubbing and touch, my husband guided me through the breathing and provided me with a circle of focus and the midwife was a constant presence of calm reassurance. It was only during pushing that I asked the RMT to stop as I felt the need to be upright and wanted pure physical support at that point. She stayed in the background after the birth, helping with the ‘clean up’ and bringing me fresh strawberries. I don’t think she said more than 10 words during the whole process and this for me was part of the beauty as she did not demand attention or care. I cannot imagine not having had her at the birth.
With our second birth, I again enlisted the services of another RMT friend but when we came to call her when it was ‘time’, we found she was ill and so could not come. We were very sad about this but we had no back up and so were left with no alternative. Honestly, I was not too worried as the midwife had a student with her and so I thought that with two of them present that there would be lots of support. However, it was so different from the first time around. The midwives were more interested indiscussing with each other as it was a teaching situation but I felt left out of the loop. This time, I felt that my husband and I were on an island alone, trying to deal with the mounting waves. The midwives were out there somewhere, outside my focus talking about things I did not or could not relate to and yet which had the potential to be scary. I don’t even remember if either of them touched me except to examine my dilation and being in the middle of labour I felt so unable to ask for more connection from them. That birth was not so smooth and I truly feel it is due to the fact that there was no ‘bridging the gap’ person there between me and my husband and what we were dealing with so intensely on the one hand, and the midwives who seemed more interested in the medical side of things than with creating an overall good vibe on the other.
With birth number 3 we knew what we wanted and what we did not want. We were prepared with the commitment of our regular RMT (with whom I had enjoyed massage throughout the pregnancy), a lovely midwife, a back-up midwife whom we had requested, and a host of labour aids. Subsequent to my first two labour experiences, I had attended two births as RMT/doula support and had experienced the positive effect of a RMT/doula presence from the other side. I was eager to try new positions, strokes, methods, etc. from the position of the receiver again and so when our RMT arrived it took very little time to start on her bag of tricks. She massaged me on the exercise ball, on the bed, in a waist-deep paddling pool that we had set up in my son’s bedroom, with her hands, with a rolling pin. It was a wonderful situation as she had a lot of birth experience and I felt extremely confident in her abilities and attitude. Unlike my first birth experience when I felt I had to be in constant communication with the RMT to express my needs, Cindy seemed to respond intuitively to my non-verbal signals, and I was not afraid of hurting her feelings if I needed to communicate a sudden aversion to a particular method. The midwife was a calm presence as well and although initially resistant in our prenatal visits to us having another professional at the birth, when it came to the ‘big event’ she could see the benefits of having someone there who could give full undiverted attention to the needs of the labourer. As wonderful as midwives are, they have a medical job to do which occasionally demands taking a step back from supporting the labourer directly to check on dilation, the baby’s heart rate, etc. She was used to doing some massage herself and so was surprised I think to see the power of the focused massage an RMT could give versus her intermittent touch. We chose our team carefully and wonderfully everyone supported each other to the fullest.
I feel extremely fortunate to have had three peaceful home births but also to have had the chance to experience different situations with regards to support. With the combination of an experienced RMT/doula, a caring midwife and family support I feel with birth number 3 we came as close as possible to the perfect experience of birth.
Pelvic girdle instability (PGI) with symphysis pubis laxity (SPL)
If the woman has this problem, she should consider giving birth in water or using all fours positions to minimise stress on the joint. Birth may be easy because the bones of the pelvis move easily; however, pain may be an issue. Bodywork is advisable for an initial pain relief option as it is best to avoid anaesthetics such as epidurals, because then the woman will not be able to feel when she is putting pressure on the bones. Often women aggravate their condition through stressing the joint in labour. If an epidural becomes necessary then it is important for the birth support people to have established beforehand how wide apart the woman can place her legs without placing strain on the pubic bone and then monitor her positions carefully.
Forceps delivery will tend to aggravate the problem as the woman will have her feet in stirrups which may excessively stress the joint. If it becomes necessary, care needs to be taken both in placing the woman in lithotomy and also to minimise the amount of time she is in the position.
If care is taken to minimise stress on the joint in labour, then the problem usually begins to resolve quickly postnatally. If the joint is further stressed during labour then it may take a long time to heal postnatally, sometimes even years, especially if appropriate support and aftercare is lacking.
10.2. Birth preparation work
This includes work preparing for birth, supporting optimal fetal positioning, and working with ‘induction’ (initiation). Working with an awareness of the position of the baby can be an important focus of bodywork during the third trimester of pregnancy and becomes increasingly important as the trimester progresses. Work with the more specific ‘labour focus’ points can be initiated from 37 weeks onwards.
Encouraging optimal fetal positioning
If the baby is in an ‘optimal’ position at the start of labour it is likely to have a beneficial effect on the progress of labour. The most beneficial position is considered to be LOA (left occiput anterior).
Encourage the woman to be aware of the position of her baby during the third trimester, when the baby begins to settle more into a particular position. She needs to be aware that she cannot ‘fix’ the baby in any position as they will continue to move right up to and during labour. As the pregnancy progresses, and the baby gets bigger, they will have more fully filled the abdominal space and are therefore able to move less. However, babies continue to shift position, especially from posterior to anterior, even during labour. Transverse babies often shift to cephalic in late pregnancy. Breech babies find it the hardest to move later on, as they need more space and research indicates that 32–34 weeks is an optimal time to encourage a breech baby to move.
Maternal position and movement may help encourage the baby to move, especially forward leaning. Work to encourage anterior cephalic positioning with the woman in forward leaning positions. The type of work to include is work to mobilise the sacrum and release the sacral uterine ligaments as tightness here may impede movement and descent of the fetus. It can be valuable to check pelvic alignment (sacrum, coccyx, sacroiliac, hips, and pubic bones). Misalignments may affect the position of the baby. The shoulders and neck compensate or reflect imbalances in the pelvis and these areas may also need mobilising/realigning in order to support good fetal positioning. Be aware, however, that for a small number of women the shape and position of the uterus and the pelvis may influence the baby’s position and it may not be possible for the baby to settle in an anterior position.
Working on an energy level will include work with the Bladder meridian. Bladder is about stimulating Water, transition and movement. Include BL 31–4 (sacral foramen points) to support releasing of the sacrum and pelvis. Include BL 67 (base of little toe) to help stimulate the baby to move. BL 67 is traditionally used with moxa for turning breech babies; however, as it stimulates fetal movement it may be used in all cases of malposition. In these other cases, holding pressures or rubbing to warm the point, or simply working intuitively all seem effective. Contrary to some beliefs, it will not turn a cephalic baby into breech.
The connection between the woman and her baby may also influence position. Encourage the woman to tune in to her baby and connect with him/her. This can be done through bodywork, visualisation, conversing with baby, writing, or artwork. If the baby is in a less optimal position then perhaps some stress is affecting it. Either the woman or baby may be afraid of the next steps in their journey. A Chinese view is that a breech baby is ‘clutching at the woman’s heart’.
Poor positioning may be partly due to modern sedentary lifestyle and certainly if the woman has a desk job, then it is important in the evening to spend time in other positions, if only resting forwards over some cushions. Even if it simply helps relieve low back ache, it will help the woman learn to relax in this kind of position which is helpful to use during labour itself.
Breech work
If the baby is breech at 32–34 weeks, encourage the woman to massage her own belly, talking to her baby and gently encouraging it to turn. This type of work can be included as part of abdominal bodywork – but it is a gentle movement. Do not attempt to rotate the baby (attempting an external version). ECV is a medical technique that needs to be done in a medical setting by primary care providers in order to be prepared should complications arise. Bear in mind that the closer to the due date the woman gets, the less room there is for the baby to turn from a breech position. If the baby is still breech at 34 weeks, a skilled practitioner can initiate moxa stimulation to BL 67. If the therapist is not trained in the use of moxa, then heat stimulation created by simply rubbing or pulling on the little toe can be effective.
One guideline for the use of moxa is the following:
Moxa BL 67 on both feet for 15 minutes, once a day for 10 days in all; initially for 5 days only, then waiting a few days and monitoring the position of the fetus, and then, if its position has not been corrected, repeating the treatment for another 5 days. It is important to pause and to monitor the position of the fetus rather than applying the treatment continuously, because the fetus may turn into the correct position and then, if the treatment is continued, may turn back into its’ previous position. Most research papers on moxibustion show that the 34th week of gestation is the optimal time to carry out the technique and gives a higher success rate.
The optimum time to start acupuncture appears to be 33–34 weeks (Cardini & Weixin 1998, Neri et al 2004). Grabowska (2005) suggests that this time is when the uterus contains its maximum amniotic fluid, and before the breech starts to descend into the pelvis.
In contrast to the advice given above, other guidance suggests that up to 10 times a day may be fine. The frequency is best determined by the woman, usually with the proviso that it should only be done if she is 100% sure that the baby has not turned. However, Betts feels that even that proviso is unnecessary as acupuncture only supports the body to do what is best for it (Betts 2006).
It is important not only to focus on more symptomatic treatment, such as the selection of only one point, but also to work with the overall energy patterns of the woman.
Many of the women with breech babies I see show signs of general heat or more commonly Heart heat, red papillae on the tongue tip. Moxa is still applicable but with cooling and calming treatment and I advise not doing the moxa within the 2 hours before bed.
(Lea Papworth)
The client needs to avoid deep squats in the third trimester if the baby is breech as they could encourage the baby to move deeper down in the pelvis, making it harder to turn.
Supporting the initiation of the birth process
It is better not to use the term ‘induction’ of labour for bodywork which is done in supporting the woman to go into labour. Changing the name of applying bodywork to energy points from ‘induction points’ to ‘initiation points’ helps to distinguish medical procedures from bodywork applications. Work is aimed at much more than stimulating hormonal release: it is about physical and emotional preparation, addressing issues that may block the woman’s comfort with going into labour, such as fear of pain, and helping to support her to move into her birthing experience with excitement, readiness, and as much confidence as is possible.
Many factors can prevent the woman from going into labour: stress, anxiety/fear, simply not feeling ready, for example not having things organised/finished, not feeling emotionally ready, or being in difficult personal or interpersonal situations. She may simply be tired, especially when so many women currently work right up to their due date. The woman may also have enjoyed being pregnant, feels very connected to her baby inside her, and is reluctant for the pregnancy to end. A holistic approach enables the therapist to discuss and consider the woman’s reality from varied angles.
While the ‘initiation’ points can be used, other strategies may also help. This may include working with the Extraordinary Vessels, general bodywork to help with relaxation and well-being and connecting with the baby. A full bodywork session is usually given addressing the many issues which may be going on for the woman, with the inclusion of ‘initiation’ points as appropriate. The focus is on supporting the woman to move from the state of pregnancy into giving birth.
Of course there are no guarantees that this work will result in turning the baby into a different position or initiate the onset of labour. However, clinically, many practitioners have witnessed success in seeing shifts in the woman’s situation, and at the very least they believe these techniques help to prepare their clients both emotionally and physically for their birthing process (Ingram et al 2005, Smith & Crowther 2004).
Before proceeding with a labour focus approach, it is important to check with the primary caregiver that there is no medical reason why the woman has not gone into labour. For example, if the baby is still high in the pelvis and is not engaged it may be unsafe to utilise techniques which could stimulate contractions.
If the baby is not in the optimal position then the first focus might be to support the baby to position itself in alignment for good descent. If the baby is in a transverse or oblique position, the labour initiation approach is unwise because unless the baby changes position there is no chance of progressing to a vaginal delivery.
‘Natural induction’ does not carry the risk of over-stimulating the uterus which could be an issue for women who have previously had a caesarean section (in contrast to induction via Syntocinon). This group of women would be carefully monitored by the primary care provider during their labour and indeed many hospitals do not perform medical induction for these clients because of the potential risk of uterine rupture. Therefore, unless there are additional factors which would make the client at higher risk for onset of labour, applying ‘initiation’ techniques should not be contraindicated for a client who is wishing to experience a VBAC (vaginal birth after caesarean).
Support for the initiation of the birth process for the woman
• Relaxation and touch encourage release of oxytocin and endorphins, which support the process.
• Energy wise, work to balance the CV and GV is important; Yin, Yang and Hormonal balance. Work with their associated points is particularly effective; KD 6 and BL 62 held simultaneously.
• Work with Girdle Vessel, to encourage it to open and using the opening and associated points GB 41 and TH 5.
• Labour focus points can be used when appropriate as they can have a strong effect on initiating the process.
• Supporting the woman/baby connection.
• Ensuring that the baby is in a good position for labour.
• Relaxed pelvis and sacrum.
Inhibitors to the birth process for the woman
It is the midbrain and the brainstem which set in motion the processes mediated by the hormones and prostaglandins. This is what is known as the ‘old part’ of the brain. Stress affects prostaglandin production; energy wise this relates to the extraordinary vessels.
Stress and adrenaline release constrict blood flow to the uterus which reduces the release of prostaglandins.
Labour focus/initiation points: SP 6, LV 3, BL 60, GB 21, LI 4
Each point has a different effect. Some women will respond to some points, because that is the effect they need, and other women will respond to other points. This means that they do not all necessarily need to be used, as only some may work. If the point is the right point for the woman, she is likely to know. It may simply ‘feel right’ and induce relaxation. It may stimulate movement of the baby and even contractions.
There is much controversy around the use of these points prior to term, based on the fear that they could stimulate miscarriage or premature labour. Indeed many people include lots of other so-called ‘forbidden points’, although these five are the most effective labour stimulation points. It is unclear why there is so much fear around the use of certain points. Simply because a point is effective in labour does not mean it will create labour in a person whose body is not ready to go into labour; that is not how energy works. However, if a pregnancy has a predisposition toward premature labour, using these points might support that inclination, although some people have anecdotally reported using these points to stop premature labour. The same is true of miscarriage in the first trimester. With a healthy gestation, there is no mechanism by which they could cause a miscarriage. Indeed, if they were that efficacious they would be widely used for supporting women in terminations. However, if the woman has an inclination for pregnancy loss, stimulating these points might add support to the process. Indeed they are useful to use in the first trimester if the fetus has died but is still inside the uterus in order to support natural miscarriage.
One of my shiatsu colleagues, A, had been trying for some time to become pregnant. Her first pregnancy ended at 9 weeks, but she did not miscarry and had to go to hospital for a dilatation and curettage. In the ninth week of her second pregnancy she began to bleed quite heavily and assumed that she must be miscarrying. She instructed her husband, a large strong man, to work all the ‘labour focus’ points as strongly and as long as he could. They worked them a lot for a day or so but A carried on bleeding and so they decided to go to hospital. A heart beat was heard, but it took several weeks for the caregivers to establish what was happening. A had a bicornuate uterus and the septum was bleeding as the uterus grew. She bled for several weeks and was hospitalised during that time. The pregnancy continued and she now has a healthy young child.
There are many anecdotal examples of therapists or women using the points because they are late with their period, and then afterwards realising that they were pregnant and carrying their babies to term. The following story illustrates how the points do not affect a healthy baby adversely.
We feel that the prohibition of these points is not especially founded in clinical reality, and it is up to each individual therapist to make their decisions regarding their use.
From 37/38 weeks the body and baby are preparing for labour and this is a time when these points are likely to be effective. They can be used as often as feels comfortable and the woman can be encouraged to practise them. A clear explanation should be given about why the points are being stimulated and the type of techniques which will be employed. If the woman does not feel comfortable with their use, do not use them. If the pregnancy is post term and medical induction is being proposed, then use these points as often and for as long as possible. In these circumstances, it is helpful to show the points to both the woman and her partner, so that they can practice them at home. The cumulative effect may be more powerful than just using them once. Try combining points. Sometimes this is more effective than using individual points but be guided by the woman. They may feel more powerful and therefore more effective. However, the combination may feel unhelpful or even strange, in which case do not proceed with them.
As ‘induction’ points they tend to be very effective. If the woman is ready to begin labour, they do not need to be stimulated much. However, the further away the woman is from labour, the more they tend to need to be worked and the less responsive they are likely to be.
Some women find some of the points helpful for pain relief during labour because they are allowing energy to flow. In labour they can be used as long and as often as the woman wants. This could be for short periods of time, or sometimes the whole of labour. Sometimes women want just one of the points held for hours. Sometimes they want different points stimulated at different stages. Each point has slightly different indications, but they all potentially help at any stage of labour, both to help labour flow and to ease pain. The best way to use them is to try them out: no harm will be caused by using the ‘wrong’ point. If a point is not effective, it will not feel right to use. Stop using it and there will be no adverse effects. Often women find that at least one of the points does help their body to focus and get on with what it needs to do: ‘labour focus’ points.
< div class='tao-gold-member'>




< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
