Stretch-tolerance Model
In clinic we may sometimes find that yoga and martial arts practitioners who are “stretch experienced” may be less concerned about painful stretching positions than those who are “stretch naïve”. This difference in attitude is the basis of the stretch-tolerance model. This model proposes that flexibility training has a psychological desensitizing influence, in which the individual becomes more familiar, less fearful and therefore more tolerant of stretching discomfort/pain.1,2 In the last decade the stretch-tolerance model has gained popularity and has been used to explain gains in flexibility following acute bouts of stretching and regular stretching, and to explain range of movement (ROM) differences between stiff and flexible individuals.3–14
A stretch-tolerance model suggests a learning process in which the individual dissociates pain from injury. Studies on conscious humans apply tensional forces that are well within tolerable pain levels. These forces are probably within safe, non-damaging ranges. Hence, the individual quickly learns that within the tolerable ranges there are no negative consequences to the stretch-pain experience (except for an occasional mild delayed onset muscle soreness (DOMS)).15 The stretch-tolerance model is in contrast to the previously held assumptions that ROM gains after stretching are the result of adaptive tissue changes.16 Although there is substantial support for the stretch-tolerance model it raises several paradoxes which will be discussed in this chapter.
This chapter will aim to answer the following questions:



Origin of Stretch-Tolerance Model
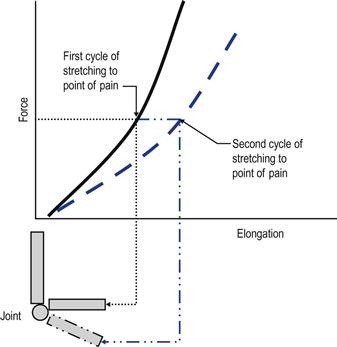
As discussed in Chapter 6, an acute bout of stretching is associated with a transient increase in tissue compliance (or reduced stiffness). This means that the joint can be stretched further using the same level of force (creep deformation). This change in stiffness would be expressed as a right shift in the force–elongation curve (Fig. 10.1). However, these viscoelastic responses are transient, lasting several minutes to an hour (Ch. 6).9 It has been assumed that regular stretching has a cumulative effect in which this right shift would become permanent, i.e. the tissue would undergo lasting changes becoming longer and more compliant.
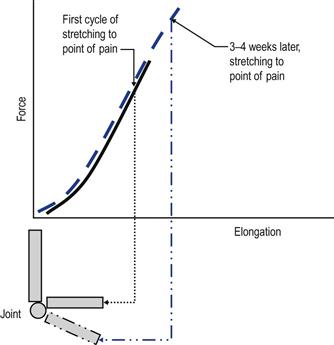
Contrary to this expectation, numerous studies demonstrated that the force–elongation profile at the onset of training remained unchanged following several weeks of stretching.5–14 A right shift was not evident following regular stretching; all that happened was that the point at which a person experienced discomfort shifted to a point further along the force–elongation curve (Fig. 10.2). These findings led to the current view that the increase in ROM is a psychological–sensory phenomenon rather than an adaptive tissue change. However, several other studies using similar testing methods have suggested that regular stretching does bring about adaptive tissue changes.16–19 So is there a reason why there is such disparity in views in studies that use similar methods?
Stiff versus Long
In normal joints a long-term increase in ROM can come about either by an adaptive reduction in the stiffness of the tissues or by an increase in their length, i.e. making the spring softer or longer. Many of the studies that support the stretch-tolerance model measured stiffness, not length (the force–elongation curve is a measure of muscle–tendon stiffness, not length). They are different measures. For example, a 1- metre rope has the same stiffness profile as a 2-metre rope, but of course they are not the same length. An alternative explanation to the stretch-tolerance model is that stiffness remains unchanged but now the muscle is longer. As a consequence the interval between pain and damage has shifted up along the curve, hence the shift in pain experience to a new tension point (Fig. 10.2). It could be argued, therefore, that the stretch-tolerance studies have demonstrated length adaptation, but instead have been interpreted as a pain tolerance phenomenon.
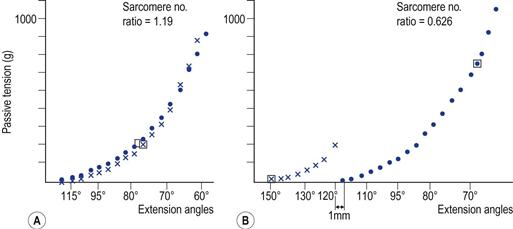
Is it possible for a muscle to undergo adaptive length change while maintaining the same stiffness? As discussed previously, paired muscle groups strive to reach a functional equilibrium at new angles of immobilization or habitual use (Ch. 4).20–22 At these angles they have to achieve optimal force production while maintaining their passive mechanical properties. Such adaptive reorganization has been demonstrated in several animal studies. In one study, immobilization of the muscle in the lengthened position resulted in a 19% increase in the number of sarcomeres in series.23 Yet there was no significant difference in the stiffness profile between the longer muscle and the control limb (Fig. 10.3). In other words, the normal muscles of the control limb displayed the same stiffness characteristics as the longer (immobilized) muscle.23 In one study, the animals were still able to maintain isometric contractions of the muscles pertaining to the immobilized joint.24 It was found that after several weeks the stiffness properties of the muscles returned to values similar to those of normal muscles, although these muscles had undergone adaptive length changes.
Further evidence supporting length versus stiffness differences comes from studies on elderly women and patients with diabetes mellitus and peripheral neuropathy. It was found that older women and patients with these conditions had an ankle stiffness profile similar to the control group. However, the older women and the patient group had a reduced ankle ROM, suggesting “shorter” rather than “stiffer” plantar flexor muscles.25,26
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


