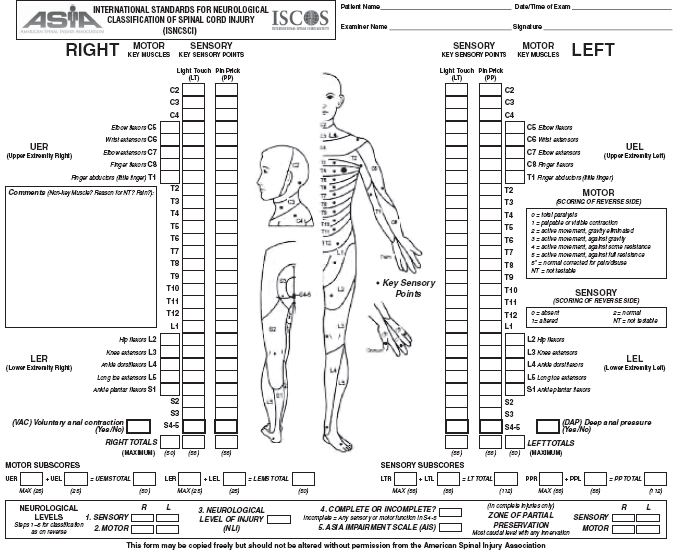
16 SPINAL CORD INJURIES Joseph E. Hornyak IV, Michael W. Wheaton, and Virginia S. Nelson Children and adolescents with spinal cord injury (SCI) must deal with the multisystem involvement imposed by the injury that is compounded by physical and psychological growth and development, which cause complications not seen in the adult. Rehabilitation is a process that extends at least until the child is physically and psychosocially an adult. Involvement by a team that is expert in the management of children and adolescents with SCIs should continue throughout this period. This chapter discusses some of the main points to be considered by those who are involved in assisting this rehabilitation process. Advances have been made in the acute management of pediatric SCI, and there is new equipment and technology for rehabilitation, but the basics of rehabilitation in this area remain the same. EPIDEMIOLOGY INCIDENCE AND PREVALENCE Compared to other disorders discussed in this text, SCI is a relatively rare disorder in the general population. The most comprehensive data on the epidemiology of SCI comes from the National SCI Database (NSCID), which is generated by the Model SCI Care Systems. The Model SCI Care Systems is a network of 28 past and current centers funded by the National Institute on Disability and Rehabilitation Research, an institute in the U.S. Department of Education. Since SCI is not a reportable condition, data collection is limited. The NSCID estimates that it collects data on 13% of the new SCI cases per year. From this data, the incidence of adult traumatic SCI is estimated to be approximately 40 cases per million in the United States, or roughly 12,000 new cases per year. This data does not include injuries that resulted in death prior to hospitalization (1). Selvarajah and colleagues used data taken from the Nationwide Emergency Department Sample from 2007 to 2009 and estimated the incidence of traumatic adult SCI to be higher at 56.4 cases per million (2). Using the same sample data set from 2007 to 2010, it was estimated the incidence of childhood and adolescent SCI presenting to emergency departments to be 17.5 cases per million, which represents 1,308 new cases per year (3). Acute SCI primarily occurs in young adults, though the average age has been rising. In the 1970s, the average age of injury was 28.7 years; since 2010, the average has increased to 42.6 years. The cause in this shift is unknown, though the incidence in SCI over the age of 60 has more than doubled since the 1980s. Other factors, such as prevention programs, advances in automobile safety, or referral patterns to Model Systems, may also be affecting the data. It was previously reported that 3% to 5% of all SCI occurred in children under age 15 and 20% of injuries occurred in those under 20. In their February 2013 report, the NSCID estimated that there were between 238,000 and 332,000 people living in the United States with SCI. DEMOGRAPHICS Publications have combined data from the Shriners Hospitals for Children and the NSCID. As in adults, males are four times more likely to have SCI than females overall, with the ratio being 1.5:1 in children under age 9 years. In children under 3 years, females have outnumbered males in some studies. The cumulative incidence of SCI in child and adolescent males was estimated to be between 2.4 to 2.8 times greater than females from the period of 2007 to 2010 (3). In younger children, there are no statistically significant racial trends. In those over age 15, there is an increased risk in African American and Hispanic American populations. These figures are all from specialized hospital data and may not represent those with milder injuries (eg, incomplete lesions and paraplegia) who are treated in smaller hospitals or in adult settings. Since the year 2010, the ethnic make-up for SCI treated in the Model Systems has been 67% White, 24.4% Black, 7.9% Hispanic, 2.1% Asian, and 0.8% Native American (1). Trauma is the primary cause of SCI, accounting for at least 93% of all SCI. Since 2010, motor vehicle crashes (MVCs) account for 36.5% of SCI, falls 28.5%, violence 13.3%, and sports injuries 9.2%. The remaining 11.4% are other and unknown causes (1). In those under age 20, violence and sports injuries are more common than falls. The sports that are most commonly associated with SCI are American football, ice hockey, wrestling, diving, skiing, snowboarding, rugby, and cheerleading (4). Hadley and colleagues (5) reviewed 122 cases of spine injury in children 16 years and younger. The median age was 15 years in males and 14 years in females. SCIs were due to MVC in 39% overall, with MVC the cause in 17% of children under 10 years of age, 26% of those 10 to 14 years, and 52% in those 15 to 16 years. Pedestrian versus MVC were 11% overall and 33%, 16%, and 3%, respectively, for the three age groups. Falls were the second leading cause under 10 years, with sports the second leading cause at ages 15 to 16 years. Fifty percent of those under the age of 10 had an occiput-C1 injury, with all levels of cervical injuries occurring in 72%, 60%, and 55% in the three age groups. Fifty percent of the subjects were neurologically intact, with bony or ligamentous injury only. More recently in 2007, Bilston and Brown (6) reported similar data from Australia, looking at children 16 years and younger. MVC accounted for 30% of all spine injuries and 50% of serious injuries. Sports were the next most common cause of all spine injuries, though falls resulted in a higher (20% vs 16%) risk of serious injury. Gender plays a significant role in the cause of injury. Violence and sports-related injuries are more common in males, while MVC injuries are less gender-specific. The authors again demonstrate that children are at higher risk for cervical spine injury, especially under the age of 8, with higher injuries occurring in younger children. Data for children and adolescents collected from a representative sample of U.S. Emergency Departments from 2007 to 2010 was reported by Selvarajah and colleagues (3). Their analysis of traumatic SCI showed a preponderance of males (72.5%) and a median age of 15 years. Those who required direct hospital admission were 62.4%, and 14.8% were transferred to another hospital for additional medical care. Traffic accidents were reported as the most common etiology of injury (37.0%) followed by falls (20.4%), struck by others/objects (16.3%), other (10.7%), firearms (8.7%), and sports (6.9%). Cervical SCI was the most common level and represented 40.5% of all injuries (19.8% high cervical and 20.7% low) and complete SCI represented less than 10% of all injuries. 14.3% of new cases of traumatic SCI in children and adolescents had a concurrent traumatic brain injury (TBI). Spinal cord injury without radiographic abnormality (SCIWORA) represented greater than 50% of all injuries. Children less than 5 years of age were more likely to be involved in a traffic accident, and have a cervical SCI that was more severe and a concurrent TBI. The incidence of SCI in sports-related injuries since 2010 is 9.2%. SCIs in American football have decreased markedly since the mid-1970s, when “spearing” was made illegal. This now-banned tackling technique resulted in a high degree of axial cervical loading. Since institution of the ban, SCI in football has decreased by 80% (7). Since the 1980s, the incidence of spine injuries and SCI has been increasing in ice hockey. These injuries are most often the result of a player being checked from behind, with his or her head down, into the boards, again resulting in high axial compression loads (8). Over the past several years, cheerleading has evolved into a competitive sport. This often involves gymnastic moves, tosses, jumps, and pyramid formations. While the incidence of SCI is low, this is a risk category where females are more likely to be injured (9). CLASSIFICATION OF SPINAL CORD INJURY LEVEL OF INJURY—ASIA IMPAIRMENT SCALE The most common method of classifying impairment from SCI is the American Spinal Injury Association (ASIA) impairment scale. The classification is based upon assessment of strength and sensation to light touch and pinprick in defined myotomes and dermatomes. Key muscle groups and sensory points are shown in Figure 16.1. The ASIA impairment scale has been modified over the years, originally based on the classification system defined by Frankel. For a child, completing the ASIA examination requires a certain level of maturity in being able to follow motor commands and respond appropriately to sensory stimulation. The examiner must take this into account when assessing children. Other factors that may limit examination (eg, long bone fractures or decreased level of consciousness) need to be taken into account as well. The motor examination scores strength on a six-point scale: 0 to 5. For each strength grade, the joint being assessed must be moved through a full available range of motion. A strength grade of 0 is given for total paralysis. A 1 is given for a visible or palpable contraction that cannot move the joint through its available range of motion with gravity removed. A grade 2 is given if the muscle group can move the joint through its range of motion with gravity removed. The joint is positioned parallel to the ground to limit the effect of gravity. A grade 3 is given when the patient can move the joint through a full available range of motion against gravity but cannot bear any additional resistance. If a patient can bear additional resistance, he or she is given a grade 4, and a grade 5 is given for normal strength. Motor scores are documented on the ASIA form and summed for a total motor score. A rectal exam must be performed to assess for voluntary contraction, and is scored as yes/no. As individual muscles are almost always innervated by multiple spinal cord levels, a strength grade of 3 is considered normal for a muscle group if the level above has grade 5 strength. This implies that the grade 3 muscle group is only partially innervated and the more proximal innervation level is intact. Sensory examination is performed using pinprick and light touch at key points, and it is graded as 0 for absent, 1 for impaired, and 2 for normal. These results are summed as well for total light touch and pinprick scores. Again, a rectal exam is necessary to assess anal sensation, also scored yes/no. The ASIA neurologic level is the most caudal segment with intact motor and sensory exam. In addition to the level is whether the injury is complete or incomplete. With a complete injury, there is no motor or sensory function in the lowest sacral segment (ie, no anal sensation or voluntary anal contraction). A complete injury is classified as ASIA-A. Incomplete injuries are classified as B to E, as listed in Figure 16.1. While an “E” is described as normal sensory and motor function, this is in the context of a previously abnormal examination. Paraplegia affects the lower extremities and, to varying degrees, the trunk. It does not affect the upper extremities; thus, T2 must be normal and any deficits are below that sensory and motor level. The preferred term from ASIA for involvement of all four extremities is tetraplegia, though quadriplegia is much more commonly used. Any injury that affects motor and/or sensation at or above the T2 level is tetraplegia. In addition, a number of syndromes have been described based upon the patterns seen after specific areas of the spinal cord have been injured. CENTRAL CORD SYNDROME The central cord syndrome was first described in 1954 (10). As its name implies, this is damage to the central area of the spinal cord. This most commonly happens in the cervical region at the lower cervical levels because of the high amount of normal motion at these segments and is often due to a hyperextension injury. Disruption of decussating spinothalamic fibers at the site of the lesion results in impaired pain and temperature sensation at those dermatomes and may also be associated with the development of neuropathic pain. Dermatomes above and below the lesion may have normal sensation. As a lesion enlarges, damage may extend into the anterior horn cells and medial corticospinal tracts, causing weakness. Reflexes may be lost at the level of the lesion as well, with possible hyperreflexia at lower levels. As this is primarily a cervical syndrome, there are typically motor and sensory changes in the arms, with relative sparing of the legs, bowel, and bladder function. FIGURE 16.1 American Spinal Injury Association Exam Sheet. Brown-Sequard syndrome results from a hemisection of the spinal cord. This is most commonly seen with low-speed penetration wounds, such as a stabbing. Corticospinal tracts and the dorsal columns cross in the brainstem, so their damage in this type of lesion leads to ipsilateral weakness and loss of vibration and position sense. The lateral spinothalamic tracts cross soon after entering the spinal cord, thus causing contralateral loss of pain and temperature sensation. ANTERIOR CORD SYNDROME The anterior (or ventral) cord syndrome is most commonly related to a vascular insult, causing infarction of the ventral spinal cord or a hyperflexion injury to the spinal cord. This injury includes damage to the corticospinal, spinothalamic, and descending autonomic tracts to the bladder. This syndrome results in paralysis, loss of pain and temperature sensation, and urinary incontinence. Vibratory and position sense, whose tracts are in the dorsal columns, are most often spared. CAUDA EQUINA AND CONUS MEDULLARIS SYNDROME Compressive injuries in the lower lumbar and sacral vertebral levels may result in damage to the cauda equina, as the spinal cord proper has terminated at a higher level. This results in scattered symptoms, depending upon which nerve roots are damaged. The cauda equina syndrome results in damage to the axon of lower motor neurons, leading to a flaccid paralysis. Conus medullaris syndrome shares many of the same features of cauda equina compression and represents damage to the bulbous, caudal portion of the spinal cord, which terminates near the L1 level. A large, nonselective lesion at this level may damage the most distal portions of the spinothalamic, corticospinal, and autonomic tracts as well as the descending nerve roots resulting in both upper and lower motor neuron findings. SPINAL CORD CONCUSSION Spinal cord concussions are an uncommon injury. These are transient injuries with full recovery. These are defined by four criteria: 1. Spinal injury with immediate neurological deficit of varying degree 2. Neurologic deficit corresponding to the level of spinal injury 3. Complete neurologic recovery within 72 hours (ASIA-E) 4. No evidence of injury on imaging These injuries are most commonly at the cervical levels. While spinal cord concussion has been reported across the age span, it is more likely to occur in children. Long-term prognosis seems excellent, though data is very limited. The mechanism of the concussion is unknown (11). SPINAL CORD INJURY WITHOUT OBVIOUS RADIOGRAPHIC ABNORMALITY SCIWORA in children has been a known entity since at least the early 20th century (12), though the acronym did not come about until 1982 in an article by Pang and Wilberger (13). The initial definition focused on children with traumatic SCI, who did not have evidence of vertebral column injury on spine x-rays, conventional and computed tomographic studies, myelograms, or dynamic flexion/extension studies. This excluded injuries caused by penetrating trauma, electrical shock, obstetric complications, and congenital spinal anomalies. In 2004, Pang published a review on what is now known about SCIWORA (14). Incidence of SCIWORA ranges between 5% and 67% of cases of pediatric SCI, with an average of 34.8%. The incidence is much higher in children 9 years and younger. Pooled data indicated an incidence of SCIWORA of 63.1% in younger children and only 19.7% in older children. Most injuries occur in the cervical cord, most commonly with C5 to C8 lesions. Thirteen percent of injuries were in the thoracic cord. This injury is thought to be primarily present in children due to the unique physiology of the developing spine, being much more mobile, without resulting in bony fractures, but causing stretch injury to other tissues. This increased mobility was thought to result in damage to the soft tissue structure of the spine, including ligamentous and neural structures, which cannot be demonstrated on radiographic studies. The advent of more advanced imaging techniques has demonstrated these soft tissue injuries. It should be noted that SCIWORA occurs in adults as well (15). SCIWORA has been reported to cause complete and incomplete SCI, as well as central cord and Brown-Sequard syndromes. Pang classified ASIA-B/C as severe injuries and ASIA-D as mild. From this pooled data, SCIWORA results in ASIA-A 22.1%, ASIA-B/C 12.6%, ASIA-D 23.2%, central cord syndrome 29.4%, and Brown-Sequard 12.7% (14). With the development of MRI, damage to the soft tissue structures in the spinal column is readily apparent. This information was recently reviewed by Yucesoy and Yuksel (16). These authors suggest that in the MRI era, SCIWORA may be an ambiguous term and that those with no lesions on neuroimaging be classified as “real SCIWORA” or spinal cord injury without neuroimaging abnormality (SCIWNA). In the strict sense, radiographs do not include MRI, yet in standard use, most practitioners would consider most imaging to fall into the category of radiograph, regardless of the nature of the physics involved in the imaging process. PROGNOSIS FOR NEUROLOGIC RECOVERY One of the most challenging aspects of rehabilitation medicine is talking with patients and families regarding prognosis for recovery. We must be able to present the best available information regarding prognosis (which is often not good) in a manner that people with varied levels of education and sophistication can understand and that can offer a reasonable and realistic degree of hope. SCI is truly devastating, and as rehabilitation specialists, we must take the impact of that into account when communicating with patients and families. We must also be aware that during these times of stress, communication may not always be effective. We must also be clear that neurologic recovery can be markedly different from functional recovery. A complete SCI examination is necessary for any discussion of prognosis. Examination at least 72 hours after injury has been determined to be a better prognostic indicator than earlier examinations (17–19). (This does not mean earlier examinations are not necessary, only that they are of less prognostic value, as they may be limited for a variety of reasons.) Most recovery from SCI occurs during the first 6 months, with a plateau reached around 9 months postinjury, though later recovery can occur. Neurologic recovery after a complete injury is poor. Ninety-six percent of those with complete paraplegia and 90% with complete tetraplegia at 1 month will remain ASIA-A. Muscle groups with a grade of 0 at initial examination, more than two neurologic levels below the level of injury, are unlikely to regain functional strength. Seventy percent of individuals with tetraplegia and a complete SCI can expect the myotome below the neurologic level to regain at least antigravity strength (20). Muscles with grades 1 to 2 have a 64% chance of increasing to functional strength in paraplegia and 97% in tetraplegia. Incomplete paraplegia has an average motor score increase of 12 points at 1 year post-injury. Seventy-six percent of those with incomplete paraplegia became community ambulators. For incomplete tetraplegia, 46% became community ambulators at 1 year (21). PREVENTION Prevention of injury is always more effective than treatment, and this is especially true in SCI. The hallmark of prevention is safety education beginning in early childhood. Use of safe equipment is the second tenet of prevention, and nowhere has this been more effective than in the use of infant and child auto restraints and adult lap and shoulder belts. This practice has also caused lap belt injuries, however, including SCIs, which are more common in children than in adults. Other prevention relating to motor vehicles is substance abuse education and laws relating to driving while impaired. Pedestrian safety is promoted almost exclusively through parent and child education. Prevention of sports-related SCIs has improved because of education, rule changes noted previously (such as no spearing in football, no checking from behind in ice hockey), better coaching, and better conditioning of players. The ThinkFirst National Injury Prevention Foundation promotes safety education. “ThinkFirst programs educate young people about their personal vulnerability and the importance of making safe choices. The message is: You can have a fun-filled, exciting life, without hurting yourself if you ‘ThinkFirst’” (www.thinkfirst.org). There are separate programs for teens and children, which promote injury prevention through talks and publications. EARLY TREATMENT SPINAL STABILIZATION Once it has been determined that the child has an SCI, the spine must be stabilized. The halo external skeletal fixation device was first described in 1968 for use in adults with cervical fractures by Nickel and colleagues (22). It has subsequently been adapted for use in children, with modifications required by the unique characteristics of the child’s skull, which is thinner. Fixation pins must be carefully placed, with attention paid to both location and depth of insertion. For thoracolumbar and lumbar fractures, nonsurgical management with a thoracic lumbar spine orthosis (TLSO) may be used either in place of or in addition to surgical stabilization (23). USE OF STEROIDS Various studies of the efficacy of the uses of methyl-prednisolone in acute SCI were conducted during the 1980s. The National Acute Spinal Cord Injury Study 2 (NASCIS 2) was published in 1990 (24), with the conclusion that patients with acute SCI treated with high-dose methylprednisolone in the first 8 hours after injury had better neurologic outcome than did those treated with placebo or naloxone. However, this was an adult study, with only 15% of patients being under 19 years of age and the youngest being 13 years old. Data are lacking in the pediatric population. A 2012 Cochrane Collaborative Review noted only eight steroid trials for acute SCI, seven using methylprednisolone. The review concludes that methylprednisolone provides some benefit (and unlikely to change prognosis for ambulation), if given within 8 hours of injury, with an initial bolus of 30 mg/kg by intravenous (IV) for 15 minutes followed 45 minutes later by a continuous infusion of 5.4 mg/kg/hour for 24 hours (25). RESPIRATORY FUNCTION Most children with SCIs have impairment of normal respiratory function because of their injuries, even in the absence of other trauma causing pulmonary problems. The basic muscles of respiration are the diaphragm, intercostal muscles, abdominal muscles, and neck accessory muscles. Any SCI that weakens one or more of these muscles impairs respiration. The child with weak or absent diaphragm function needs ventilatory support. If the diaphragm is functional but intercostal and abdominal muscles are weak or nonfunctional, the child will need assistance with coughing and respiratory secretion management and may need ventilator support during respiratory illnesses or during sleep. If the child only has weakness of the abdominal muscles, assistance with coughing may be the only respiratory support needed. All children with acute SCI should have respiratory function evaluated. At the very least, this evaluation should include chest radiographs and measurement of oxygen saturation and end-tidal carbon dioxide or arterial blood gases. If the child is able, forced vital capacity and inspiratory and expiratory forces should be measured on a daily basis until the child is medically stable. Because the child with SCI has restrictive respiratory dysfunction (so-called bellows failure), not lung disease, the earliest pulmonary abnormality will be hypercarbia and not hypoxia. End-tidal carbon dioxide measurement is a simple noninvasive way to follow hypercarbia over time, and may be useful for outpatients as well as for inpatients. URINARY FUNCTION Most children with acute SCIs develop a neurogenic bladder. During spinal shock the bladder is initially flaccid, and may subsequently become spastic or dyssynergic. Flaccid bladders need to be drained either continuously or intermittently. Because indwelling catheters are associated with infections, the child should be converted to a clean intermittent catheterization program as soon as there is no medical reason to have continuous monitoring of urine output. Spastic or dyssynergic bladder management is discussed in further detail later in this chapter. GASTROINTESTINAL AND BOWEL FUNCTION After acute SCI, the gastrointestinal tract usually stops functioning initially, thus requiring the use of nasogastric decompression. Once the ileus has resolved and the child is taking enteral feeding, a bowel program should be instituted, with the ultimate goal of continence without impaction. The consistency of the stool is normalized through the use of fluids, fiber, and enteral medications, as needed. Evacuation is assisted through the use of digital stimulation, enemas, and/or rectal medications. FLUIDS AND NUTRITION Careful attention must be paid to fluid balance and nutrition in the child with an acute SCI. A balance must be maintained between adequate hydration for intravascular volume/blood pressure, soft stool, and over hydration which may cause bladder distension, leakage and need for increased catherization. To promote healing, the child must also receive adequate nutrition. A common standard is to start some form of nutrition within 24 hours of injury. Typically, this is parenteral nutrition initially, followed by either oral or tube feedings when the ileus is resolved. For some children who have the ability to eat orally, refusal to eat may be the only way they have of controlling their medical treatment, so nutritional intake should be closely monitored during the acute and rehabilitation hospitalizations. REHABILITATION Rehabilitation of the child with SCI is a lifelong process that starts soon after injury. It does not start and end with admission to and discharge from a rehabilitation unit, and this must be made clear to the patient and family. Goals of rehabilitation will be dependent upon a number of factors, primarily the patient’s age, level and completeness of injury, and amount of neurologic recovery. Rehabilitation of the child with SCI is comparable to rehabilitation of the child with any other acute change in function, usually with less need for cognitive rehabilitation. The entire rehabilitation process should focus on the whole child in the context of his or her family and community, and be performed by a rehabilitation team of professionals that focuses on the needs of children. It should be noted that on occasion, some older children may be more appropriate for an adult rehabilitation service, while some young adults or people with cognitive impairment may be better served on a pediatric rehabilitation service. When older children are treated on an adult service, it is important that the appropriate pediatric, social, and education services be available. Goals for rehabilitation should include maintenance or attainment of good health and prevention of secondary complications, while promoting maximal and age-appropriate functional independence. The focus of rehabilitation can range from primarily family education (eg, C4 or higher complete tetraplegia with ventilator dependence) to primarily complete patient functional independence (eg, T10 complete paraplegia). The goals of rehabilitation will change as the child matures. Table 16.1 lists expected functional goals for levels of SCI. MOBILITY Mobility for the child with SCI begins with the process of learning to sit again. Sitting is compromised as a result of the lack of neurologic control of the trunk related to the SCI, impairments in the autonomic nervous system, and physiologic adaptations to deconditioning during the acute hospitalization. Hypotension and syncope can result. Support hose, wrapping of the lower extremities with elastic bandages, and abdominal binders may help maintain blood pressure. Progression to sitting is a gradual process and should be started as soon as possible to minimize deconditioning. Short periods of sitting as tolerated can be done multiple times during the day, gradually increasing the duration of the time up. Early use of a power or manual wheelchair (as appropriate) is encouraged. It is important to monitor insensate skin as the duration of time up increases to minimize the development of pressure ulcers. The use of pressure-relieving cushions or periodic pressure-relieving maneuvers is critical. Patients will begin working on bed mobility, rolling in bed, and transferring from the bed to the wheelchair. As the patient improves, more advanced transfers will be the main focus of physical therapy interventions. Standing and walking, either with orthoses or independently, will be done as appropriate. Table 16.2 shows mobility guidelines from recommendations by the American Academy of Orthopaedic Surgeons and Shriners Hospitals for Children. It should be noted that often younger children with high lumbar or thoracic paraplegia may be ambulators with appropriate bracing. As with paraplegia from myelodysplasia, it is not unusual for these children to become more wheelchair-dependent as they reach adolescence. Ambulation at these levels is quite energy-inefficient, while the use of a wheelchair is very efficient. This later use of a wheelchair should be discussed with the patient and family well before it occurs so that it is seen as the expected path and not as a failure of the patient or family.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


