Specificity in ROM Rehabilitation
Often individuals (as well as animals) overcome their injury and range of movement (ROM) losses by taking actions that resemble the movement patterns which they have lost: a person with a sprained ankle will attempt to gradually walk; a tennis player with a shoulder injury will attempt to gradually return to playing tennis. Similarly a patient with a frozen shoulder, given time and without any rehabilitation, will often regain their full ROM by daily use of their shoulder.1 This behaviour can be considered to be Nature’s “gold standard” for movement recovery – practise what you aim to recover.
However, in physical therapy we provide a curious management. Patients are often given exercise that has no resemblance to the movements that they wish to recover. This raises the possibility that what is prescribed in clinic may not provide the most effective ROM rehabilitation. For example, would floor exercise or manual stretching of the hip improve stride length?
This chapter will explore the following topics:
 Can commonly prescribed stretching exercise improve functional activities?
Can commonly prescribed stretching exercise improve functional activities?
 Can manual stretching techniques improve functional activities?
Can manual stretching techniques improve functional activities?
 What kind of gain is expected to carry over from the ROM challenge to functional activities?
What kind of gain is expected to carry over from the ROM challenge to functional activities?
 How close to the goal task does the ROM challenge have to be?
How close to the goal task does the ROM challenge have to be?
 What factors can improve the carry-over between ROM exercise and functional activities?
What factors can improve the carry-over between ROM exercise and functional activities?
Specificity and Generalization
In order to understand how to transform clinical gain into functional improvement we need to look at the specificity phenomenon in adaptation.
When we learn a new skill the motor, tissue and physiological adaptation is specific to that particular task (specificity).2–8 This allows the task to be optimally performed with minimal energy expenditure, physical stress and error. This adaptation is unique, and optimized for that particular activity, but may be unsuitable for a different activity.9–12 This is why the performance of cross country skiing does not improve by dancing practice.13 However, if specificity in adaptation was absolute it would mean that we would have to learn the task as well as each of its infinite variations. This problem in adaptation is overcome by our ability to carry-over learning or training experiences to variations of the same activity/task (generalization). So once a movement has been learned it can be performed with many variations without having to practise them all.14–17 Hence, throwing a ball can be performed in conditions that have never been encountered during the training. Similarly, we can drive an unfamiliar hired car without having to re-learn driving.
The generalization–specificity principle in learning and training has important implications for therapeutic stretching. In many stretching approaches it is expected that particular techniques or exercise will help to improve a wide range of functional activities. An example is core stability exercise in which specific trunk muscle training is believed to enhance performance in many different sports and daily activities. Similarly, there is a common expectation that stretching techniques would improve a variety of daily activities. For example, muscle energy technique (MET) applied to shoulder extensors would be expected to improve many functional overhead tasks.
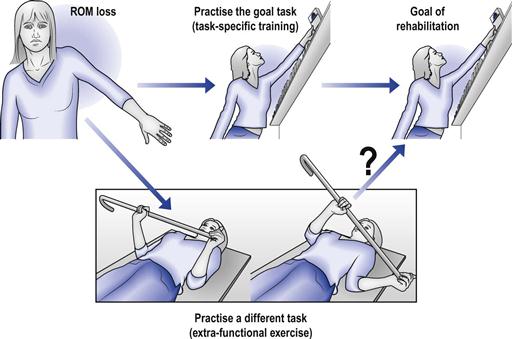
On the other hand, specificity implies that the treatment has to closely resemble the goal activity,18,19 i.e. walking should be rehabilitated by walking, standing by standing and balance by balancing. Equally, ROM challenges should replicate closely the movements being recovered; for example, shoulder ROM should be challenged during functional overhead activities (Fig. 5.1). Specificity implies that, if the stretching and goals of rehabilitation are dissimilar, there would be an ineffective carry-over of clinical gains to functional improvements. For example, it would be expected that MET of shoulder extensors would be ineffective in improving functional overhead activities. This is because there is no resemblance between the muscle recruitment sequences during MET and those of a functional movement such as reaching overhead.
From a therapeutic perspective, a generalization principle is very attractive and therefore prevalent in physical therapies; all that is needed is a particular set of universal exercises to improve a wide spectrum of daily activities. On the other hand, a specificity principle means that treatment has to focus on a wider selection of affected activities. The specificity–generalization issue is not well researched in physical therapies, and for answers we need to look at motor learning and training principles, in particular at the transfer principle in training.
Transfer of training
Imagine a clinical situation in which a patient with flexion contracture of the hip is given particular exercises to recover hip ROM; say, kneeling on all-fours quads stretch. The ultimate aim is to influence hip function during walking rather than improve the performance of this particular exercise. By prescribing such exercises we assume that there are some elements within the exercise that would generalize and carry-over to improve walking. This carry-over is called transfer; it is how the performance of a particular task (say, walking) is influenced by practise of another activity (quads stretch exercise).10,20–22
In physical therapies it is often assumed that several elements can be transferred between the exercise and the goal task; using hip exercise as an example (Fig. 5.2):




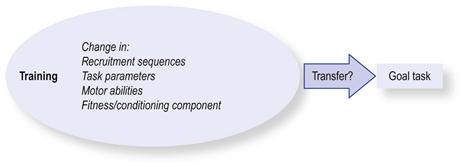
The question that emerges is which of these movement elements can transfer between the exercise and the goal task? To answer this we need to look at the distance which the movement elements have to carry over, i.e. how close is training to its goals.
Measuring similarities
To explore resemblance we need some form of yard-stick to “measure” this distance. This can be assessed by looking at whether the training is within the same task (within-task), e.g. train in walking to improve walking, or between two dissimilar tasks (between-task), e.g. training on all fours to improve walking.
An example of exercise that aims to utilize within-task transfer is the common use of weights during walking or running. Here, the training and the task resemble each other but with the added overloading of force. Within-task transfer is represented in ROM rehabilitation by the expectation that improvement of force in one range would carry over to other, unpractised ranges.
Between-task training aims to improve a particular task by training or treating in a different task; for example, the common practice of balancing on a Swiss ball in order to improve balance during walking. Here, the focus is on balance transfer but the exercise is dissimilar to the goal task (walking). Another example would be to train for explosive force by vertical jumps (one task), but with the aim of improving sprinting (another task), an activity that also requires an explosive force. Between-task transfer is represented in ROM rehabilitation by the expectation that practising the all-fours hip extension exercise on the floor would improve walking hip ROM.
A further measure of resemblance is similarity and dissimilarity of the movement patterns between the exercise and the target task.23,24 For example, does the movement of the leg during all-fours leg extension exercise resemble the movement patterns of the leg during walking?
Whether the training is within-task or similar provides four categories for assessing the “distance” between the ROM challenges and the goals of rehabilitation. The challenges can be (Fig. 5.3):




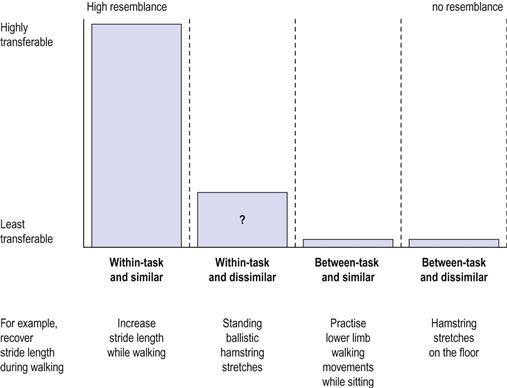
FIGURE 5.3 Assessing similarity and transferability between the training and the rehabilitation goals.
Imagine again the patient who has reduced hip extension that limits walking. The training would be within-task–similar if the person is instructed simply to walk with a wider stride. Another possibility is to walk while performing pelvis-stabilizing exercises. In this case, the movement is within the task of walking but is somewhat dissimilar to it (within-task-dissimilar). Performing leg movements that resemble walking while sitting would be an example of an exercise which is between-task-similar. The rehabilitation would be between-task and dissimilar to walking if the patient is instructed to perform a hip extension exercise while lying prone.
Now that we have a way of measuring resemblance we can explore in which of these categories transfer is most likely to occur.
Studies of Specificity and Transfer
Overall, several decades of studies in motor learning suggest that specificity is the dominant outcome of training/practice and transfer between tasks is mostly absent and if present is considered to be insignificant.25–32
Specificity in movement can already be observed in young children.5 It seems that each task in their movement repertoire is learned specifically, with little or no transfer between tasks that share the same motor abilities. For example, dynamic balance skills do not transfer to static balance skills and vice versa. A high level of fine motor control in the hand may help in drawing but not in playing with Lego bricks, an activity that also depends on fine motor control. This lack of transfer of motor abilities between tasks has also been shown in adults.25,33
Some within-task transfer has been shown in sports training but it tends to be modest and unpredictable. Sprinting performance was shown to improve by single-leg horizontal jumps but not by vertical jumps using both limbs, such as jump squats.18 Transfer may fail to occur even in trainings that seem to closely resemble the task. For example, resistance sprint training using a towing device fails to improve sprint performance.34 Similarly, off-ice skating exercises do not improve on-ice performance in speed skaters.35 Even activities that look identical, such as sprinting and endurance running, each have their unique, non-transferable knee force–angle profiles. This specificity is also observed anatomically. The fascicle length of leg muscles is greater in sprinters than in distance runners.36,37 That is why marathon runners are not great sprinters, although the movements they perform in running look very similar.
Even in within-task training some elements of the task parameters may not transfer well. For example, the gains of resistance training at one speed may not transfer well to another speed of the same movement.38–41 Strength gains are greatest at the training velocity with some carry-over to other velocities.42 Similarly, strength gains are greatest at the training angles with some transfer to other ranges (see more below).43–45
There is substantial evidence demonstrating that between-task training gains do not transfer well. Core stability exercises fail to improve sports performance (between-task-dissimilar).46–48 Different forms of resistance exercise have failed to improve specific sports activities such as football kicks, sprinting, netball, hockey, throwing velocity in water polo and rowing.18,49–55 Even resistance training in one particular posture may not transfer strength gains to other postures.56
In elite gymnasts, athletes, judo competitors and dancers, training to hold difficult, sport-specific postures does not transfer balance ability to commonly used unspecific standing postures.57–60 Cross-training by cycling does not improve running and may even reduce running economy.61–63 Training in isolated tasks, such as hip flexibility or trunk-strengthening activities, does not improve the economy of walking or running.64 Vertical jumps are improved by training in vertical but not by training in sideways jumps.65 Upper limb resistance exercises do not improve arm coordination,66 and so on.
All these studies provide a very clear message: the greater the distance in resemblance the less likely is the transfer. Optimal training gains occur when the training is within-task and similar to its goals. Least effective are between-task and dissimilar training. But what about stretching? How likely is it to provide performance gains?
Transfer in stretching
Most traditional stretching exercises represent training which is between-tasks and dissimilar to its goals (Ch. 1). Hence, we would not expect transfer to occur. Indeed, regular and warm-up stretching, in all its variations, has failed to demonstrate transfer of gains to sports performance.67–69 One study demonstrated that 4 weeks of contract–relax stretch training (proprioceptive neuromuscular facilitation) of the knee improved flexion range but did not alter the active movement performance (peak isokinetic quadriceps torque).70 In another study, 10 weeks of lower limb stretching had no effect on vertical jumps.71 Similarly, 6 weeks of passive static stretching and contract–relax stretching improved the ROM but neither had any significant effect on the drop jumps.72 In contrast, one study has shown that 8 weeks of upper limb passive stretching was shown to improve bench presses.73 However, a recent review found no benefit in acute bouts of static stretching for any form of muscular performance.69
These studies suggest that traditional, extra-functional stretching approaches are unlikely to provide performance gain because of their dissimilarity to the goal task. But what about ROM challenges that are within-task? Is generalization possible? Would an improvement in shoulder control of 0–90° flexion improve the control of other ranges, say, 90–120°? Or would improvements in reaching range in the frontal plane be generalized to improvement of the same movement but in the coronal plane?
Motor learning studies suggest that learning a task in one range can generalize/transfer to other angles of the same task. This was demonstrated in a study in which subjects had to catch a series of light and heavy balls with either a “bent” or a “straight” arm configuration.32 It was found that the learning of catching in one configuration transferred 100% to the other. Here, the contents of transfer are the recruitment sequences of the movement (see Transfer of Training). Force training in one range seems to be angle/ROM specific.43–45 However, there may be some carry-over of force gains to other untrained angles,42 in particular if the full range is practised rather than specific angles.29,31
In summary, optimal transfer and generalization occur when the ROM challenges are within-task and similar to the movement goals. The four movement parameters, force, range, speed and endurance, are the most likely elements to be transferred or generalized during task-specific training.
Studies of Specificity and Transfer in Patients
So far this chapter has explored the specificity in healthy individuals. The question that remains is whether adaptation principles apply to individuals with pathological ROM losses. In a limited number of studies transfer of rehabilitation gains has been examined in patients with musculoskeletal injuries and pain conditions and in patients with central nervous system damage.
In individuals suffering from chronic neck pain, extra-functional neck exercises do not transfer to improvement in functional head–neck movements (between-tasks and dissimilar).74 In contrast, a positive transfer of postural stability was demonstrated in a study of balance in subjects with lateral ankle sprain. Training under moderately unstable conditions transferred to improvements in postural control under more challenging stability conditions (within-task-similar).75 However, we do not know whether these improvements would transfer to functional activities outside the research lab.
For stroke patients resistance cycling or seated strength exercise improves strength in these activities but has little or no effect on walking;76,77 sitting and reaching training improves sitting and reaching and the production of vertical force through the leg as they lean forward.78 The vertical force improvement in the leg seems to transfer to improvement in getting up from sitting, but nothing from that training transfers to walking. However, training of stroke patients in walking improves walking speed and distance but not balance.79–81 Balance seems to be improved by challenging balance.82,83 But challenging static balance in standing might not transfer well to dynamic balance during walking.84 So here, too, transfer can be unpredictable and finicky.
Studies of individuals with age-related or pathological ROM losses suggest a lack of transfer between tasks. One study of postmenopausal women found no effect of regular exercise and stretching on walking performance.85 In one study of older individuals with hip flexor contracture, 8 weeks of hip and ankle stretching provided a modest improvement in passive ROM (hip 6.8°, ankle 3.5°) but failed to improve stride length.86 In a similar study, 10 weeks of hip and ankle stretching improved hip flexibility (1.5°) but failed to show significant improvements in gait performance. Twelve weeks of foot exercise that included ankle stretching failed to improve physical gait performance in elderly individuals.87 In a recent study passive stretching was shown to increase passive hip ROM (5°) and stride length (by 2.7 cm) during comfortable but not during fast walking speeds.88 However, at neither walking speed was there any improvement in peak hip extension or peak anterior pelvic tilt, i.e. there was no transfer of hip flexibility from the exercise to the walking.89,90 This is likely to be due to the failure to emulate the complex intermuscular coordination of the hip during walking by passive stretching (Ch. 8). It would have been useful in all these studies to include a task-specific group that trained in walking faster or with a wider gait.
In 2011, a Cochrane systematic review reported that various forms of traditional stretching for contractures failed to improve functional activities.91
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


