Partial Scaphoid Excision of Scaphoid Nonunions
Rafael J. Diaz-Garcia
Joseph E. Imbriglia
DEFINITION
Scaphoid fractures are quite commonplace, representing the most frequently fractured carpal bone with an annual incidence of approximately 29 per 100,000.5 Fractures of the scaphoid, when treated acutely and appropriately, have union rates greater than 90%.3,9 However, without proper diagnosis and treatment, scaphoid fractures frequently result in nonunion.
Initial treatment for a scaphoid nonunion is typically open reduction and internal fixation (ORIF) with bone graft, be it a corticocancellous wedge or a vascularized graft.
Despite appropriate internal fixation and bone grafting, failure rates are approximately 15% in waist fractures and 33% in proximal pole fractures.12
If ORIF and bone grafting fails, the surgeon is then left with difficult choices.
Salvage procedure which may have a higher rate of satisfactory results
Silicone prostheses previously described have had poor results due to silicone synovitis and implant loosening, dislocation, and breakage.13
ANATOMY
The scaphoid bone represents the bridge between the proximal and distal rows of the carpus. It is tilted in both the volar and radial planes in respect to the central axis of the forearm, articulating with both rows.
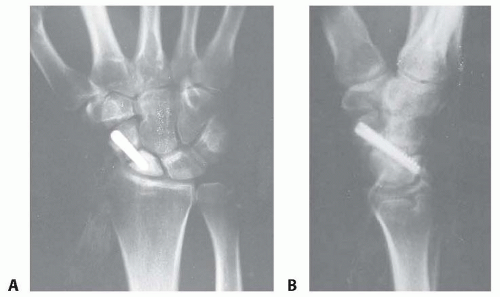
FIG 1 • Failed ORIF of a scaphoid nonunion (PA and lateral views).
The scaphoid is mostly covered in articular cartilage and has important intrinsic and extrinsic ligamentous attachments.
Most of the vascular supply to the scaphoid enters the bone distal to the waist and perfuses in a retrograde fashion (FIG 2).6,17
The proximal pole is most at risk secondary due to its tenuous blood supply.
All of these anatomic features make surgical management complex.
PATHOGENESIS
Patients with scaphoid fractures who present with delays (>4 weeks) in both diagnosis and treatment can develop a nonunion. Other risk factors for nonunion include proximal fracture location, comminution, fragment displacement or angulation, and associated carpal instability. As with other fractures, smokers are at increased risk for nonunion.
Acute scaphoid fractures with fracture fragment displacement more than 1.0 mm, an intrascaphoid angle more than 45 degrees, or a height-to-length ratio more than 0.65 have a higher incidence of nonunion.18
Because the scaphoid serves as a bridge between the proximal and distal carpal rows, a scaphoid fracture can severely disrupt wrist biomechanics and normal loading patterns.
Scaphoid fractures disrupt the normal linkage between the two rows, and thus the proximal fragment remains with the lunate via the scapholunate ligament and the distal fragment flexes unimpeded.
Scaphoid collapse reduces the carpal height and allows the lunate to rotate in a dorsal intercalated segmental instability (DISI) pattern.
Scaphoid nonunion advanced collapse (SNAC) arthritis develops from the altered biomechanics.
NATURAL HISTORY
Most patients with scaphoid fractures, and thus nonunions, are young males between the ages of 20 and 30 years.5,7
There is controversy regarding the true natural history of patients with scaphoid nonunions given that most studies are biased toward symptomatic patients.8 However, it is widely believed that radiographic signs of posttraumatic arthritis will develop in almost 100% of patients with a scaphoid nonunion. These degenerative changes occur in a predictable pattern, and the process may take 5 to 20 years.8,10,14
Arthritis first develops between the distal pole of the scaphoid and the radial styloid (SNAC wrist stage I; FIG 3A).
Left untreated, stage I SNAC will progress to involve the midcarpal joint (SNAC stages II and III; FIG 3B,C).
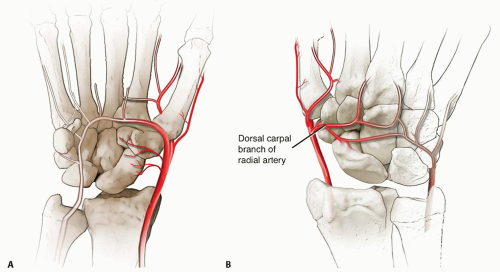
FIG 2 • A. Volar intraosseous blood supply to the scaphoid with laterovolar and distal vessels visualized. B. Dorsal intraosseous blood supply to the scaphoid.
Many patients present once pain and decreased range of motion in the wrist has become increasingly severe. In these cases, salvage procedures requiring arthrodesis are often the only options left.
PATIENT HISTORY AND PHYSICAL FINDINGS
Related posts:
 Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Vascularized Bone Grafting and Capitate Shortening Osteotomy for Treatment of Kienböck Disease
Operative Treatment of Metacarpal Fractures
Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Vascularized Bone Grafting and Capitate Shortening Osteotomy for Treatment of Kienböck Disease
Operative Treatment of Metacarpal Fractures
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


