Exposure and Scheduling the ROM Challenge
Recently, I was standing on a beach and observing the wide range of sports activities that individuals were undertaking, in particular their warm-up routines. Whether they were about to run, swim or surf they all exhibited a similar warm-up behaviour. For a brief period, lasting no more than a few seconds, they stretched specific body areas. Further down the beach were a couple of people practising yoga. Their activity was strikingly different. Their movements were slow and, once in position, they sustained it for periods that ran into minutes. Presumably, both groups aimed to achieve a similar goal of maintaining or improving agility. Yet, increased flexibility is more likely to occur in one training condition than in the other, but which is it, and what is the optimum exposure for stretching?
This chapter explores the scheduling factor of the range of movement (ROM) challenge: the duration (single session), frequency (how often repeated) and time span (weeks/months), collectively termed here exposure. It will aim to provide answers to commonly raised question about the scheduling of stretching:
 What is the optimum duration for ROM challenges?
What is the optimum duration for ROM challenges?
 How often should ROM challenges be repeated?
How often should ROM challenges be repeated?
 Can clinical stretching or exercise provide sufficient exposure?
Can clinical stretching or exercise provide sufficient exposure?
 How does scheduling of stretching change in the presence of pathology?
How does scheduling of stretching change in the presence of pathology?
 Is there a scheduling difference between traditional and functional stretching approaches?
Is there a scheduling difference between traditional and functional stretching approaches?
Duration of Challenge
The scheduling of the ROM challenge depends largely on the intrinsic physiological processes that underlie adaptation. From a physiological perspective there is probably some ideal frequency and duration that would optimize mechanotransduction. However, this quantity is currently indefinable, partly because of the lack of research but also because of the numerous extrinsic influences that can affect this process, such as the nature and extent of the ROM pathology, the type of tissue affected and metabolic factors.
Currently, most of the information about scheduling of stretching is derived from studies of healthy young individuals. Many of the studies used passive stretching approaches, with a duration ranging from 6 to 60 seconds often quoted as being the most effective.1–8 In the hamstrings, a daily episode of stretching for 30 seconds was found to be more effective than 15 seconds. However, there are no significant differences between stretches lasting 30 and 60 seconds,3,4 implying that the most effective duration is about 30 seconds. This has become the unofficial duration standard for passive stretching; well, at least for the hamstring muscles.9 Interestingly, increasing the stretching duration to 30 minutes per day, over several weeks, fails to provide any additional ROM gains.10–12
The 30-second duration creates a paradox. It implies that yoga practitioners and dancers might be wasting valuable training time. According to research, 30 seconds should suffice. Yet, runners who stretch for short periods are rarely able to perform the agility feats associated with flexibility training. Perhaps for adaptive changes we need to look at longer duration and extended time spans – scheduling practices that are observed in flexibility training. So the relationship between stretching exposure and gains in flexibility remains unresolved in healthy individuals. But the important question here is what happens to the stretching exposure in the presence of a ROM pathology? Does 30 seconds suffice or does it need to be raised considerably?
Duration in the presence of ROM pathology
It seems that, in the presence of pathology, the duration of stretching has to increase dramatically. It was demonstrated that 6–12 hours of daily splinting is required to overcome flexion contractures in the proximal interphalangeal joint after surgery, and more days spent in the cast resulted in greater ROM improvements (60° at 3 days and 106° at 6 days).13,14 Another study suggested that 8–12 hours per day for 8 weeks are necessary to effectively overcome similar contractures.15 This phenomenon was also demonstrated in frozen shoulder, in which maximizing the total time spent at end-ranges tends to improve ROM.16 In patients with contractures due to central nervous system damage, it is estimated that over 6 hours of daily stretching would be required to improve ROM.17,18 Several studies have explored shorter duration in patients with spinal cord injuries. ROM challenges were applied daily to the ankle for 30 minutes, over time spans of 4, 6 and 12 weeks using either passive stretching or static standing on a wedge.10,19,20 ROM improvements were not observed in any of these studies.
These studies suggest that, in the presence of pathology, ROM challenges may have to occupy up to half of the person’s waking day, which of course is unattainable unless splints are used. Even if these studies overestimated the stretching duration by 2–3 times we would still be unable to fulfil this exposure quota. Is there a solution?
Competition in ROM adaptation
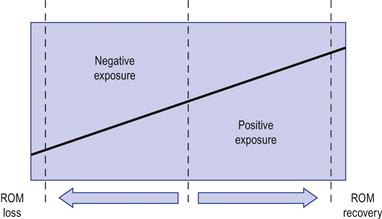
Perhaps we should look at the exposure component in a different way altogether, and consider that ROM loss and recovery represent a competition in adaptation between the pathological process that maintains the condition and the ROM challenges that counteract it (Fig. 7.1).
As discussed previously, musculoskeletal adaptation tends to be specific to support movement efficiency and efficacy. Given two competing environments or training regimes, adaptation is likely to occur in the one the individual is most exposed to. This is why body-builders will find yoga difficult to perform and vice versa. It is also why those who train for flexibility need extensive stretching exposure to compete with the adaptation imposed by their daily activities. Hence, dancers seem to be in a constant state of stretching (I have seen a dancer sitting in a side-split at an air terminal while waiting for a flight, and the flight was delayed!). The question is what happens to this competition when an individual has some pathological condition which is competing with the ROM challenges?
Let us re-examine the post-surgical studies which suggest that several hours of daily splinting are required to overcome contractures. This can be viewed as a competition in adaptation between the post-surgical pathology that maintains the tissue shortening and the splinting that promotes tissue elongation/extensibility. Since the pathology that maintains the shortening is present for 24 hours per day, it is likely to win this one-sided competition, unless the duration of ROM challenge is increased dramatically. As discussed above, this would be almost impossible to attain clinically or even by exercise, so is there some other practical solution?
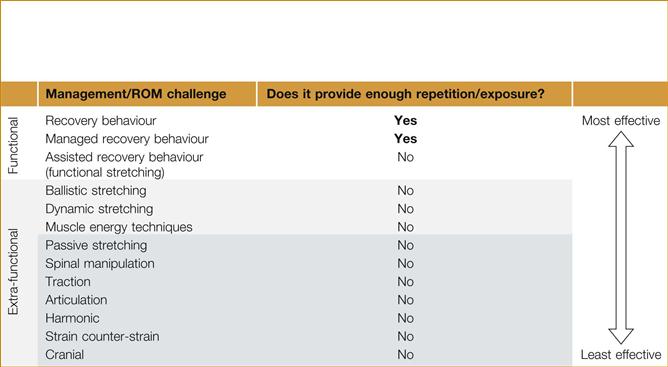
The solution is to tilt the competition in favour of the ROM challenge. This can be achieved by making the ROM challenges a part of the person’s habitual daily activities. For example, while writing this chapter, an elderly patient consulted me about a severe shoulder sprain that took place 2 weeks previously. During that period, the patient kept her arm in a sling and close to her body at all times, which resulted in a rapid loss of glenohumeral ROM (see fear avoidance, Ch. 11). Her shoulder ROM increased dramatically, and within days of the initial session, by the simple instruction to keep the arm away from the body during daily activities. The emphasis was to amplify daily tasks that promote such ROM challenges as often as possible over behaviour that favoured shortening. This does not exclude the use of specific exercises; however, from an exposure perspective, they would have a lower therapeutic value than persistent functional ROM challenges (Table 7.1).
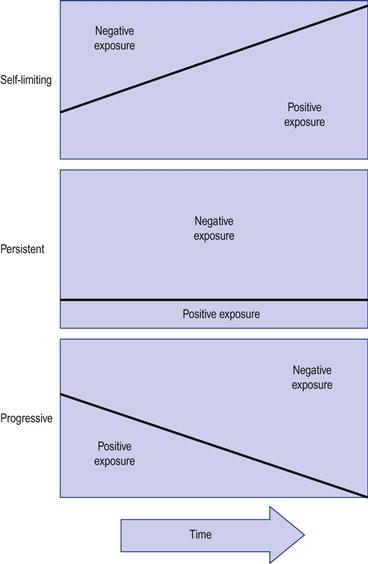
A competition in adaptation also means that ROM rehabilitation is more likely to succeed in self-limiting conditions (as the “negative” competition is gradually receding); it will have to be permanently maintained in persistent conditions (“negative” competition maintained) and ineffective in progressive conditions in which the “negative” competition is increasing (Fig. 7.2).
Ratio between maintaining and recuperating signals
A competition in adaptation suggests that there is an ideal ratio between the duration of ROM challenge and the behaviour that maintains the ROM loss.
In animal studies even short periods of passive stretching have been shown to compete with the deleterious effects of immobilization. In one of the studies the animals’ limbs were immobilized in a shortened position using a sports tape.21 Daily, the tape was removed and the limb was placed in the lengthened position and immobilized in this position using the same taping method. The immobilization duration ranged from 15 minutes to 2 hours. At the end of the lengthening procedure the animal was re-immobilized in the shortened position. It was found that 15 minutes daily of elongation was insufficient to counteract the loss of sarcomeres in series. Increasing the duration to 30 minutes daily increased the numbers of serial sarcomeres to pre-immobilization levels. Progressively longer duration of stretching resulted in further increases in the number of serial sarcomeres. In a similar immobilization study, even 15 minutes of stretching every second day was shown to be sufficient for normalizing the ratio of connective tissue to muscle fibres.22,23 Shorter durations, such as a 40-minute stretch once a week, were not sufficient to prevent the loss of serial sarcomeres.24
These studies suggest that the competition in adaptation does not have to be in the same ratio, i.e. an hour of immobilization does not have to be matched by an equal duration of elongation. Clinically, it is impossible to estimate this ratio. The simple solution is for the patient to use the recovery behaviour as frequently as possible during the day. Is there a danger of overexposure to ROM challenges? Probably not: the more exposure, the better.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


