Upper Extremity
General Upper Extremity Guidelines
In evaluating upper extremity (UE) impairment, there are four prime elements to consider:
Diagnosis-based estimates (DBEs)
Amputation
Nerve injury: (a) loss of sensation, (b) loss of motor function
Loss of motion (not on a neurologic basis)
Sometimes a fifth element is also involved:
Other (miscellaneous) conditions: arthroplasty, instability, deformity, weakness, vascular compromise, pain
The five elements are evaluated as explained in the following subsections.
Diagnosis-based Estimates
DBEs are estimated impairment ratings for common medical procedures or problems. Table 6-1 (shown later in this chapter) is a quick reference for common upper extremity impairments using DBEs. All values in this table are stand-alone; that is, they are not to be combined with any other values for the same joint, injury, or problem, with the exception that if the individual exhibits more than the usual loss of motion for the condition, the value may be combined with an impairment from the loss of motion table for that joint.
If Table 6-1 is not used, all impairments for a given joint or body area can be combined, other than as noted in the exceptions discussed later in this chapter.
Amputation
Use the amputation table (Table 6-2) or Figure 6-1. (All figures and tables mentioned in these subsections can be found in the section “Rating Specific Upper Extremity Impairments,” later in this chapter.)
Neurologic Injury
For a digital nerve injury, determine digital sensory loss from Figure 6-2. If the nerve injury is proximal to the digits, use Table 6-3.
TABLE 6-1 Diagnosis-Based Estimates for Common Upper Extremity Procedures | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 6-2 Amputation, Upper Extremity | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
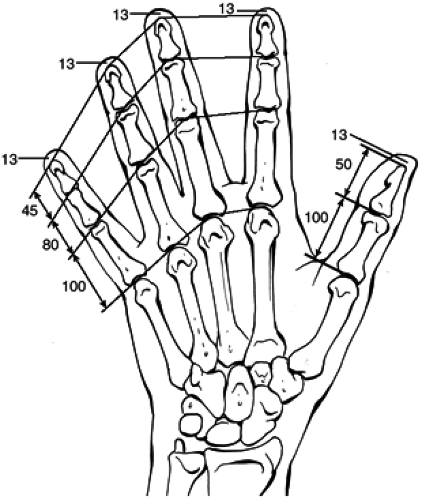 Figure 6-1. Chart for amputation of a digit, showing percentage of impairment. |
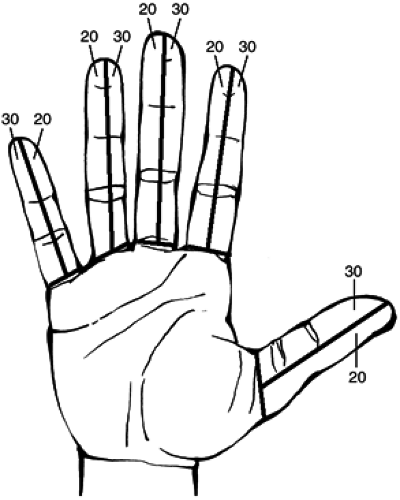 Figure 6-2. Digital sensory loss chart showing percentage of digital impairment for total digital nerve loss. |
TABLE 6-3 Nerve Injury, Upper Extremity | |||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||
Loss of Motion
Motion loss measurements should be active measurements (i.e., active on the part of the patient). Amazingly, active versus passive range of motion measurements are not addressed in the AMA Guides. However, consultants on this issue unanimously agreed that active motion is the parameter of most importance. After all, what benefit does a patient with a 45-degree arc of wrist dorsiflexion gain if the motion is purely passive and the individual must use a brace to position the hand in space?
For loss of motion due to stiffness, musculotendinous malfunction, or skeletal problems, use Table 6-4 for the thumb, Table 6-5 for the index or middle finger, Table 6-6 for the ring or little finger, Table 6-7 for digital deformity, Table 6-8 for digital values,
Table 6-9 for the wrist, Table 6-10 for the elbow, or Table 6-11 for the shoulder. If neurologic impairment is the cause of loss of motion, do not use a loss of motion table.
Table 6-9 for the wrist, Table 6-10 for the elbow, or Table 6-11 for the shoulder. If neurologic impairment is the cause of loss of motion, do not use a loss of motion table.
TABLE 6-4 Loss of Motion: Thumb | |||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


