Upper Extremity
Median Nerve
(Fig. 3-1)
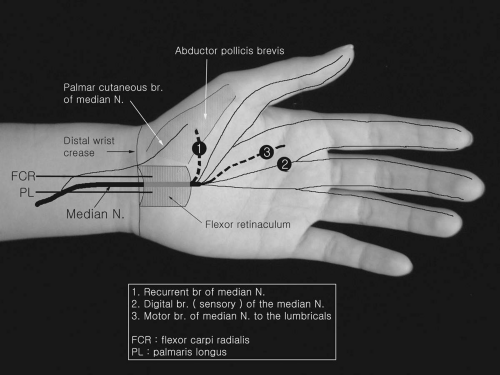 Figure 3-1. Anatomy for median nerve conduction studies. |
Median Nerve Motor Conduction
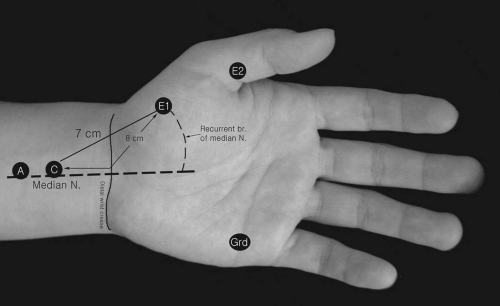 Figure 3-2. Median nerve motor conduction study to the abductor pollicis brevis. |
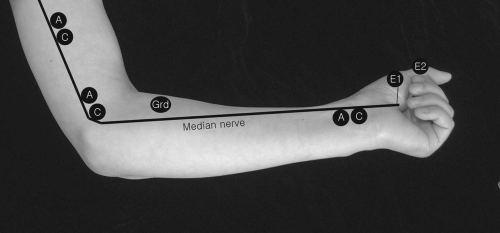 Figure 3-3. Median nerve stimulations at the wrist, elbow, and midarm. |
Recording Electrode Placement
E1 The active recording electrode (E1) is placed on the most prominent eminence of the thenar area halfway between the midpoint of the wrist crease and the midpoint of the first metacarpophalangeal joint in the volar aspect. Thus, the E1 electrode is placed over the motor point of the abductor pollicis brevis (APB).
E2 The reference recording electrode (E2) is attached on the proximal phalanx of the thumb.
Stimulation
Wrist Stimulation is applied 8 (or 7) centimeters (cm) proximal to the E1 at the wrist, between the tendons of the flexor carpi radialis and palmaris longus.
Elbow The stimulator is positioned in the medial aspect of the antecubital space (crease), just lateral to the brachial artery.
Axilla This stimulation can be done between the biceps brachii and triceps muscles.
Erb’s point (supraclavicular fossa) This stimulating point is located in the supraclavicular fossa, about 2 cm above the clavicle. Surface stimulation of the lower trunk, the origin of the median nerve to the APB, often is technically difficult because this trunk is located too deep.
Reference Values1
N = 47
Conduction velocity (m/s) | Amplitude (mV) | |
|---|---|---|
3.7 ± 0.3 | 56.7 ± 3.8 | 13.2 ± 5.0 |
Korea University Medical Center (KUMC) (unpublished) N = 64
Conduction velocity (m/s) | Amplitude (mV) | |
|---|---|---|
3.3 ± 0.4 | 57.4 ± 2.7 | 9.5 ± 2.7 |
Comments
Before using any reference data, the author’s recording instrumental parameters should be reviewed. High-intensity stimulation on the nerve may spread the currents to inadvertently stimulate the ulnar nerve at the wrist, elbow, or axilla.
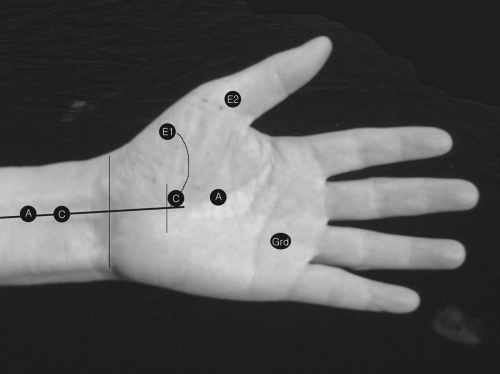
Median Motor Nerve Conduction with Midpalm and Wrist Stimulation
Recording Electrode Placements
E1 and E2 electrodes: The APB muscle and proximal phalanx of the thumb.
Stimulation
Comments
This method can determine whether there is any conduction block or delay of the median motor fibers as they pass the carpal tunnel area. The midpalm stimulations may show the following inadvertent effects: (a) activation of the ulnar nerve’s deep branch; (b) direct stimulation of the motor point of the APB; (c) baseline distortion due to shock artifacts. Care must be taken so that the shapes of compound muscle action potentials (CMAPs) with both wrist and midpalm stimulations are similar.
Martin-Gruber Anastomosis (Median-to-Ulnar Anastomosis)
Recording Electrode Placements
Comments
Anatomy: anastomosis is usually of the median nerve branching to ulnar nerve in the forearm (rarely ulnar to median).
Recognized easily in CTS (carpal tunnel syndrome) cases.
Unusually fast conduction velocity of the median motor nerve in the forearm.
In cases of severe CTS, wrist latency to the APB may be slower than the elbow latency to the APB with initial positivity of CMAP configuration with elbow stimulation.
In ulnar nerve motor NCS (nerve conduction study), ADM (abductor digiti minimi)-CMAP amplitude is larger with above elbow stimulation than with below elbow stimulated ADM-CMAP recordable with median nerve stimulation at the elbow.
One of two main anomalous innervations (Martin-Gruber, accessory peroneal nerve) is documented well in EDX (electrodiagnosis).
Martin-Gruber anastomosis occurs in 15% to 25% of patients.
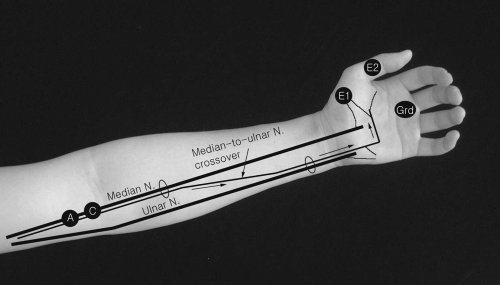 Figure 3-5. Anatomy of Martin-Gruber anastomosis. |
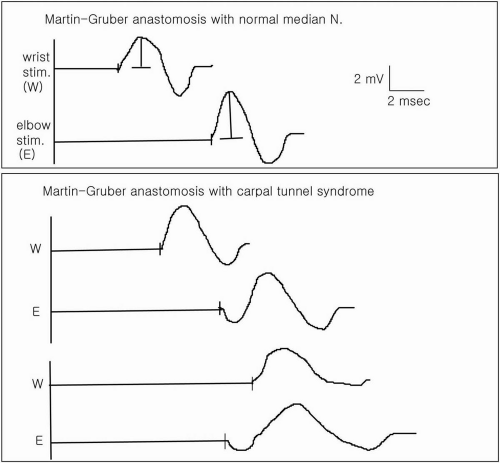 Figure 3-6. Typical tracings of anomalies with median nerve conduction studies. |
Median and Ulnar Nerve Conduction to the Second Lumbrical and First Palmar Interosseous
Recording Electrode Placements
E1 The E1 is positioned in the midpoint between the second and third metacarpal bones in the palm side.
E2 The E2 is placed on the proximal phalanx of the second digit.
Stimulation
The stimulations of the median and ulnar nerves are performed at the wrist (Fig. 3-7).
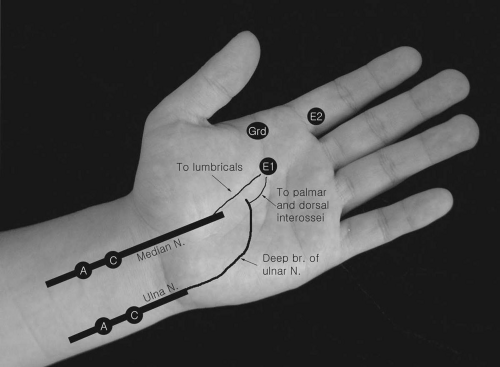 Figure 3-7. Median and ulnar nerve conduction studies to the second lumbrical and first palmar interosseous. |
Comments
Supramaximal stimulation with surface electrode in the palm requires greater intensities than that of the wrist because the nerves are located more deeply under the thick palmar fascia and subcutaneous fat pad. This may lead to potential errors in measurement of motor conduction parameters (latency, amplitude, and morphology) because of inadvertent shock artifact or stimulus spread. However, this inching technique is highly sensitive to uncover the focal conduction abnormalities even mild sensory and/or motor fiber demyelination.
Anterior Interosseous Nerve Conduction to the Pronator Quadratus
Recording Electrode Placements
A standard concentric needle serving as E1 and E2 is inserted into the pronator quadratus about 2 cm proximal to the ulnar styloid process and between the space of the ulnar and radius bones in the dorsal aspect of the forearm (Fig. 3-8).
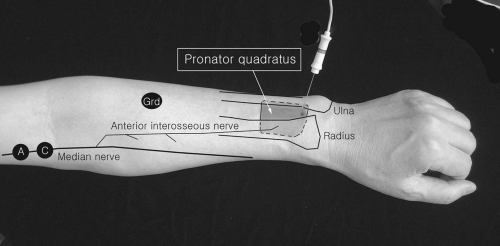 Figure 3-8. Anterior interosseous nerve conduction study to the pronator quadratus with needle electrode recording. A concentric needle is inserted into the pronator quadratus through a space between the ulna and radius in neutral forearm position. |
Mysiw and Colachis2 used surface electrodes for recording.
Stimulation
The stimulus is applied just above the elbow between the medial epicondyle and biceps tendon, just lateral to the brachial artery.
Anterior Interosseous Nerve Conduction Study to the Flexor Pollicis Longus
Recording Electrode Placements
Stimulation
Stimulation can be applied proximally at the elbow, just medial to the brachial artery.
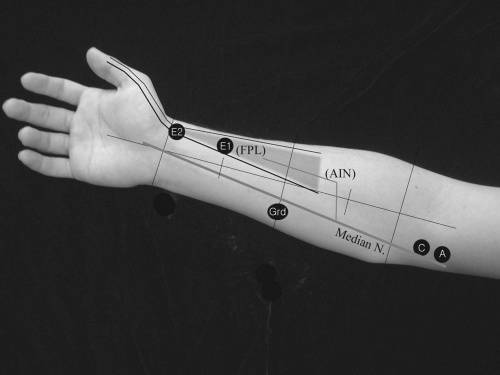 Figure 3-9. Anterior interosseous nerve conduction to the flexor pollicis longus. |
Reference Values
Latency (ms) | Amplitude (mV) |
|---|---|
2.6 ± 0.4 (1.8 to 3.6) | (5.6 ± 1.2) (3.8 to 7.5) |
No fixed distance (9.1 to 10.2 cm) was used.
Latency (ms) | Amplitude (mV) |
|---|---|
3.6 ± 0.3 | 6.9 ± 1.1 |
(3.1 to 4.1) | (5.4 to 10.0) |
Recording Electrodes:
1 cm × 2.5 cm strip surface electrode was used for both E1 and E2; E1 was placed transversely over the distal portion of the flexor pollicis longus, 7 to 10 cm proximal to the distal wrist crease; E2 was applied over the lateral aspect of the wrist; median nerve stimulation was applied 18 cm from E1 at the elbow.
Comments
The shape of CMAPs often shows initial positivity and a rather complex form, likely due to a volume-conducted response from adjacent median nerve-innervated muscles. Care must be taken not to overstimulate the nerve at the elbow.
C-8 Root Stimulation with Monopolar Needle Electrode
Recording Electrode Placements (Fig. 3-10A)
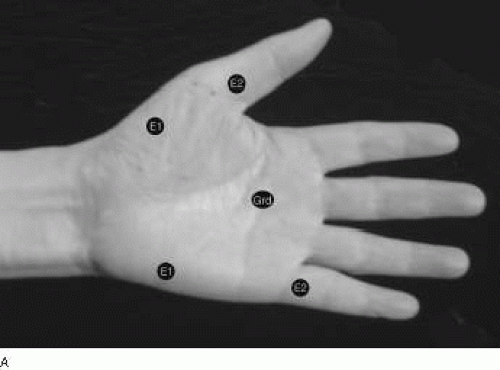 Figure 3-10. A: CMAPs recording at the abductor pollicis brevis and abductor digiti minimi with C8 spinal root stimulation. B: C8 root stimulation. |
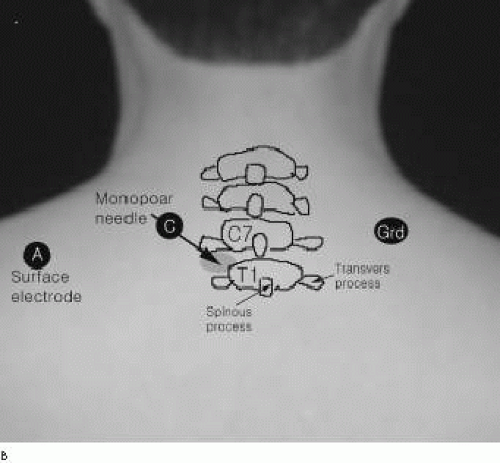 Figure 3-10. (continued) |
The recording E1 and E2 are placed on either the abductor digiti minimi or the abductor pollicis brevis.
Stimulation (Fig. 3-10B)
To stimulate the C8 nerve root, a monopolar needle (Teflon coated) is placed between the C7 and T1 transverse processes, 1 to 2 cm lateral to the C7 spinous process, and a surface electrode as anode is arranged 2 to 3 cm lateral to the stimulating needle electrode. For measuring the conduction velocity, the distance between the C7 spinous process and the E1 recording electrode is measured.
Comments
Comparison of the side-to-side latency difference may be useful to assess the proximal conduction abnormalities of the C8 root.
Median Nerve Sensory Conduction Study (Fig. 3-11)
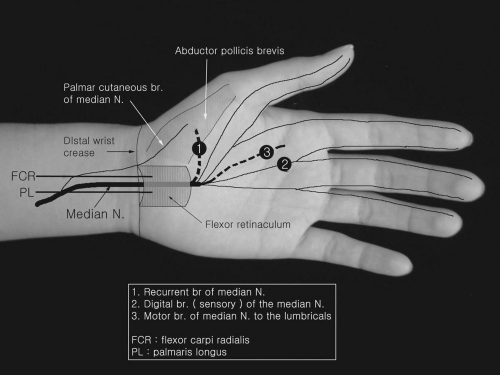 Figure 3-11. Anatomy for median nerve sensory conduction studies. |
Median Nerve Sensory Conduction to the Third-Digit—Antidromic Techniques6
Recording Electrode Placements (Fig. 3-12)
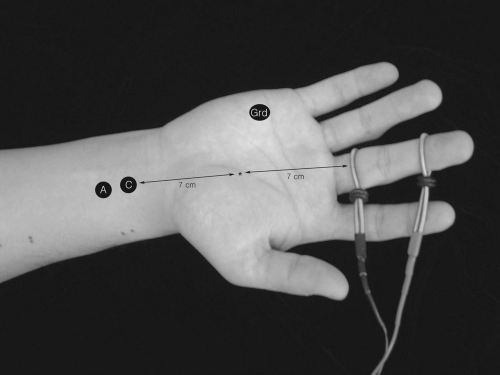 Figure 3-12. Median nerve sensory conduction to the third digit. |
Antidromic median sensory nerve conduction studies can be performed with any of the four digits (digit I to IV). Using ring, clip, or bar electrodes, the sensory nerve
action potentials can be recorded. When bar electrodes are used, the distance between the active and reference electrodes are fixed.
action potentials can be recorded. When bar electrodes are used, the distance between the active and reference electrodes are fixed.
E1 In routine median sensory conduction, the E1 electrode is placed on the midpoint of either the second or third digit. We prefer the third digit recordings. The E1 placement requires some separation from the metacarpophalangeal joint to avoid volume-conducted muscle responses from the activated adjacent hand intrinsic muscles innervated by the median nerve.
EMG Machine Settings
Stimulation Sites
Wrist (Fig. 3-12) Stimulating cathode with anode proximal is placed 14 cm proximal to the E1 at the wrist between the tendons of the flexor carpi
radialis and palmaris longus and ideally proximal to the distal wrist crease. Supramaximal stimulus is applied to the median nerve.
Midpalm The stimulation is applied 7 cm distal to the point of wrist stimulation at the midpalm, ideally distal to the carpal tunnel. On the midpalm stimulation, a short distance between the stimulating cathode and recording electrodes and higher stimulus intensities may evoke a distortion of sensory potentials due to shock artifacts. Rotation of the anode to the cathode in the palm may help to minimize the distortion.
Elbow Stimulate the median nerve just above the crease of the antecubital fossa and medial to the biceps tendon at the elbow.
Comments
Measurement parameters include the onset and negative peak latencies and amplitude (baseline-to-negative peak) of compound sensory nerve action potential.
Normal values7 | ||
|---|---|---|
Conduction velocity (m/s) | Amplitude (μV) | |
3.2 ± 0.2 | 56.9 ± 4.0 | 41.6 ± 25 |
7 Johnson EW, Melvin JL: Sensory conduction studies of median and ulnar nerves. Arch Phys Med Rehabil 1967;48:25-30. | ||
Korea University Medical Center (KUMC) (unpublished) N = 43 Age 53.3 ± 9.1 (years old)
Stimulation site | Latency (ms) (to negative peak) | |
|---|---|---|
Wrist (14 cm) | 3.3 ± 0.2 (2.9 to 3.8) | 36.5 ± 8.3 (24 to 55) |
Midpalm (7 cm) | 1.8 ± 0.1 (1.6 to 2.0) | 48.6 ± 10.9 (33 to 75) |
Median and Ulnar Nerve Sensory Conduction Studies to the Fourth Digit
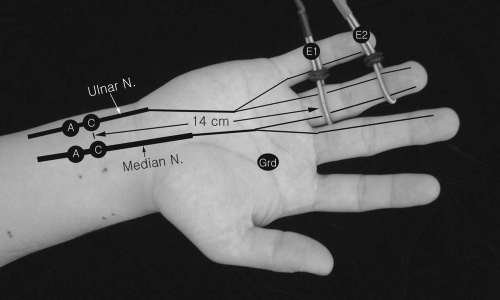 Figure 3-13. Median and ulnar sensory nerve conduction studies to the fourth digit. |
Recording Electrode Placements
E1 and E2 Ring or bar electrodes are placed at the midpoint of the proximal phalanx in the fourth digit.
Stimulation
The stimulation is performed 14 cm proximal to the E1 at the wrist for both median and ulnar sensory nerves.
Comments
Comparison of latencies between the median and ulnar nerves is helpful to assess early or mild carpal tunnel syndrome. Significant latency difference between the median and ulnar nerves, ≥0.5 ms.
Median and Radial Sensory Conduction Studies to the Thumb
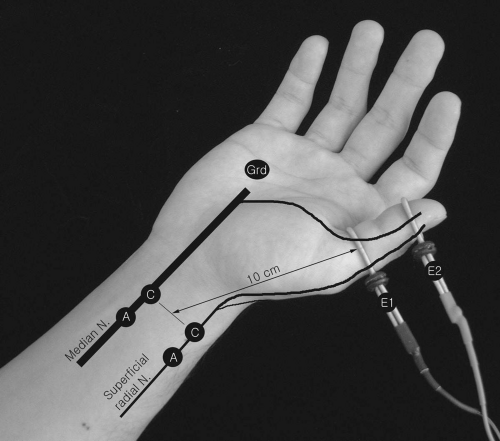 Figure 3-14. Median and radial sensory nerve conduction studies to the thumb. |
Recording Electrode Placements
Stimulation
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


