This article describes 2 nonsurgical approaches to the treatment of carpal tunnel syndrome that are not routinely offered, probably due to a lack of awareness. Osteopathic manipulative treatment (OMT) is commonly used for many medical problems, including musculoskeletal issues. OMT of the carpal tunnel is well described and researched, and can be clinically used by a skilled practitioner. The second treatment strategy is a more recent development. The use of ultrasound for guidance of injection is established, but a newer technique using sonographically guided percutaneous needle release of the transverse carpal ligament has shown promising results.
Key points
- •
There is a wide range of treatment strategies for carpal tunnel syndrome (CTS), from conservative to surgical, with varying degrees of supportive evidence that must be considered. The choice of treatment is complicated by clinical severity, chronicity, and patient preference.
- •
Osteopathic manipulative treatment of the carpal tunnel is well described and researched, and can be clinically used by a skilled practitioner.
- •
Sonographically guided percutaneous needle release of the transverse carpal ligament has shown promising results.
Introduction
Of the challenging pain syndromes discussed in this issue, carpal tunnel syndrome (CTS) will be the most commonly encountered by the physiatrist. After a clinical diagnosis is made and, if necessary, electrodiagnostic or ultrasonographic testing is performed (see the article entitled “Carpal Tunnel Syndrome Diagnosis” by Sucher and Schreiber elsewhere in this issue), treatments to consider include conservative and surgical strategies, with varying degrees of supportive evidence. The choice of treatment is complicated by clinical severity and chronicity of the disease, and patient preference. Typical treatment options include, but are not limited to, splinting, occupational and/or physical therapy, nutritional support, anti-inflammatory regimens (including injection), and ergonomic modifications, all of which should be considered in carefully selected patients. This article highlights 2 nonsurgical approaches to treatment that are not commonly used, probably because of a lack of awareness. Osteopathic manipulative treatment (OMT) is often used for many different medical problems, including musculoskeletal issues that practitioners tend to link to spine care. In fact, OMT for CTS is well described and researched, and can be clinically used by a skilled practitioner. The second treatment strategy has been more recently developed with the increased use of ultrasonography as a therapeutic imaging tool, and application of its diagnostic capabilities described in the article entitled “Carpal Tunnel Syndrome Diagnosis” by Sucher and Schreiber in this issue. The use of ultrasound for the guidance of injection is established, but a newer technique using sonographically guided percutaneous needle release of the transverse carpal ligament (TCL) has promising results. OMT of the carpal tunnel and sonographically guided percutaneous needle release of the TCL are described herein.
Introduction
Of the challenging pain syndromes discussed in this issue, carpal tunnel syndrome (CTS) will be the most commonly encountered by the physiatrist. After a clinical diagnosis is made and, if necessary, electrodiagnostic or ultrasonographic testing is performed (see the article entitled “Carpal Tunnel Syndrome Diagnosis” by Sucher and Schreiber elsewhere in this issue), treatments to consider include conservative and surgical strategies, with varying degrees of supportive evidence. The choice of treatment is complicated by clinical severity and chronicity of the disease, and patient preference. Typical treatment options include, but are not limited to, splinting, occupational and/or physical therapy, nutritional support, anti-inflammatory regimens (including injection), and ergonomic modifications, all of which should be considered in carefully selected patients. This article highlights 2 nonsurgical approaches to treatment that are not commonly used, probably because of a lack of awareness. Osteopathic manipulative treatment (OMT) is often used for many different medical problems, including musculoskeletal issues that practitioners tend to link to spine care. In fact, OMT for CTS is well described and researched, and can be clinically used by a skilled practitioner. The second treatment strategy has been more recently developed with the increased use of ultrasonography as a therapeutic imaging tool, and application of its diagnostic capabilities described in the article entitled “Carpal Tunnel Syndrome Diagnosis” by Sucher and Schreiber in this issue. The use of ultrasound for the guidance of injection is established, but a newer technique using sonographically guided percutaneous needle release of the transverse carpal ligament (TCL) has promising results. OMT of the carpal tunnel and sonographically guided percutaneous needle release of the TCL are described herein.
Osteopathic manipulative treatment of CTS
OMT is an essential component of the conservative management regime for CTS. Various manual techniques have been proved to be effective. Training to develop proficiency in OMT for CTS is not difficult for clinicians; especially those skilled in manual medicine. Sucher and colleagues have determined the most effective techniques to elongate the TCL, thereby increasing volume within the carpal tunnel (CT) and decreasing pressure on the median nerve (MN). The OMT described is a powerful and effective form of nonsurgical decompression of the MN at the CT.
Indications
Patients may be considered for this treatment if they fulfill the following criteria:
- 1.
Clinical diagnosis of CTS. It is not required that the patient have electrodiagnostic testing before the procedure, although the authors recommend testing whenever possible to confirm diagnosis and rule out other causes. The finding of mechanical restriction over the carpal canal by palpatory diagnosis is the primary indication for applying OMT at this site (see the article by Sucher and Schreiber elsewhere in this issue).
- 2.
Osteopathic principles guide physicians to evaluate the entire musculoskeletal system, then apply treatment to all areas of somatic dysfunction d
d Somatic dysfunction is defined as the impaired or altered function of related components of the somatic (bodywork) system including: the skeletal, arthrodial, and myofascial structures, and their related vascular, lymphatic, and neural elements.
diagnosed by appreciation of tissue-texture change, asymmetry, restriction, and tenderness (TART findings). Therefore, exclusive focus on the CT could ignore other important areas of restriction that affect wrist and hand function. Proximal dysfunction will affect biomechanical behavior distally, and should be addressed (but is beyond the scope of this article).
Contraindications and Precautions
- •
Focused OMT can be administered vigorously without concern of injuring the MN by specifically avoiding direct pressure over the CT ; this is not a problem if the manipulating fingers work along the edges of the CT.
- •
Arthritic changes in the first carpometacarpal joint can limit the degree of range of motion necessary to create sufficient traction along the TCL, thus preventing adequate stretch or elongation of the ligament.
- •
Fragile skin can cause ecchymosis, especially on the dorsal hand. Inadvertent counterforce applied on the dorsal aspect of the hand by the operator’s manipulating fingers can injure the skin and lead to bruising. Vigorous force is required to successfully elongate the TCL.
- •
Any increased pressure on a badly damaged nerve could lead to more axon loss. However, severe cases of CTS do not respond well to conservative treatment or surgery. There is the distinct possibility that vigorous application of manipulative forces, even for brief periods of time, could further injure a fragile nerve that has already sustained axon loss. The caveat is that severe CTS may not improve with surgery, and not all patients want surgery. Severe CTS is a relative contraindication, and requires clinical judgment combined with patient participation (informed consent).
Techniques
Anatomy
Descriptive terminology used to identify movement through the anatomic planes can vary somewhat in the literature. The terms applied for the techniques described herein are consistent with the specific literature referenced for application of OMT in CTS.
Osteopathic manipulative treatments
- 1.
Transverse extension (TE): Fig. 1
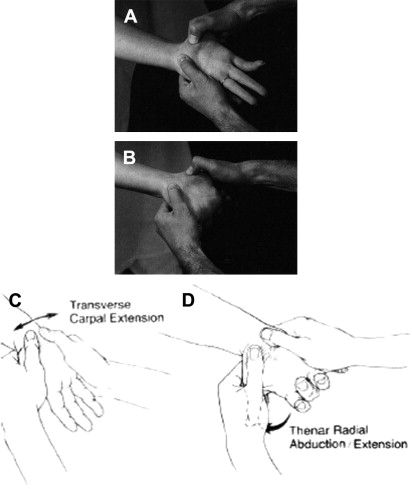
Fig. 1
Manipulation for carpal tunnel syndrome (CTS): transverse extension (TE) of the carpal tunnel and thenar abduction/extension. ( A ) Operator’s fingers (not visible beneath patient’s hand) press upward on the dorsal part of the patient’s wrist (centrally). Operator’s thumbs apply pressure along the attachment edges of the transverse carpal ligament (TCL) at the medial and lateral borders of the carpal bones. In addition, the patient’s thumb is grasped firmly by the operator’s right hand and pulled into radial abduction with extension. ( B ) Same technique as in A , except the patient’s wrist and digits are hyperextended, further opening or extending the canal, and the operator’s thumbs have progressed away from midline, stripping the ligamentous and myofascial attachments back. ( C ) TE. Action-line arrows demonstrate movement of thumbs apart to widen the carpal tunnel. ( D ) Graphic of thenar radial abduction with extension. Action-line arrow demonstrates the movement of the thumb required to release the abductor pollicis brevis and opponens pollicis muscle attachments at the TCL.
([ A, B ] From Sucher BM. Myofascial release of carpal tunnel syndrome. J Am Osteopath Assoc 1993;93:92–4. © 1993 American Osteopathic Association. Reprinted with the consent of the American Osteopathic Association; and [ C, D ] From Sucher BM. Palpatory diagnosis and manipulative management of carpal tunnel syndrome. J Am Osteopath Assoc 1994;94:647–63. © 1994 American Osteopathic Association. Reprinted with the consent of the American Osteopathic Association.)
- 2.
Thenar extension and abduction (ThEA): Fig. 1
- 3.
Hyperextension (wrist and digits): Fig. 1
- 4.
Opponens roll (thenar): Figs. 2 and 3
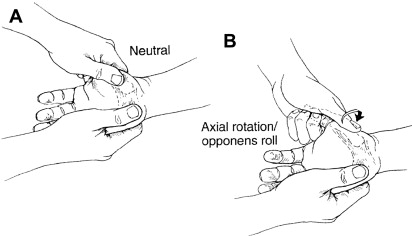
Fig. 2
Manipulation for CTS: opponens roll maneuver. ( A ) Relaxed or neutral position. ( B ) Thenar abduction with extension and lateral axial rotation (retroposition).
( From Sucher BM. Palpatory diagnosis and manipulative management of carpal tunnel syndrome. J Am Osteopath Assoc 1994;94:649. © 1994 American Osteopathic Association. Reprinted with the consent of the American Osteopathic Association.)
Fig. 3
Manipulation for CTS: opponens roll maneuver of the carpal tunnel in a cadaver; view of distal aspect of carpal canal. ( A ) Stretch position for the abductor pollicis muscle into radial abduction and extension pulls TCL taut, up against the median nerve (MN), identified by arrow marked N-D, and electromyogram electrode. Notice pressure effect just distal to edge of ligament (identified by arrow marked TCL). ( B ) The more superficial abductor has been dissected away. Thumb is pulled back into radial abduction with extension, and lateral axial rotation has just been initiated. Opponens pollicis muscle (identified by arrow marked O) and its ligamentous attachment are pulled taut, slightly contacting the MN. ( C ) Opponens roll. Maximum axial rotation is introduced, rotating thumb laterally (notice change in position of operator’s fingers around thumb). Observe how the still taut ligament is now elevated up off the MN with slight “gapping” even as ligament is being stretched.
( From Sucher BM. Palpatory diagnosis and manipulative management of carpal tunnel syndrome. J Am Osteopath Assoc 1994;94:649. © 1994 American Osteopathic Association. Reprinted with the consent of the American Osteopathic Association.)
- 5.
Guy-wire (GW): Fig. 4
Fig. 4
Manipulation for CTS: guy-wire (GW) maneuver and TE. ( A ) GW technique applied to cadaver limb, dissected with ligament cut away, to illustrate the flexor pollicis longus tendon (FPLT) deflected around the inner edge of the trapezium (T) and flexor digitorum porfundus-5 tendon (FDP5T) deflected around the inner edge of the hamate (H), creating a fulcrum effect, tending to pull apart the carpal arch ( thin black arrows ). The electromyogram electrode (needle) identifies the MN centrally. ( B ) Combination TE with the GW manipulation technique. The GW maneuver is performed by an assistant holding the thumb and little finger while the physician applies distal-row TE.
( From Sucher BM, Hinrichs RN. Manipulative treatment of carpal tunnel syndrome: biomechanical and osteopathic intervention to increase the length of the transverse carpal ligament. J Am Osteopath Assoc 1998;98:685. © 1998 American Osteopathic Association. Reprinted with the consent of the American Osteopathic Association.)
- 6.
Combination maneuvers: Figs. 1 , 4 B and 5
Fig. 5
Manipulation for CTS: all techniques combined. The wrist and digits are hyperextended ( central palmar green arrow ) against the operator’s knee, transverse extension is applied by the operator’s thumbs ( short transverse blue arrows on either side of the wrist), opponens roll lateral axial rotation is applied by the operator’s left hand ( short curved yellow arrow on the left), and the GW maneuver is applied by both of the operator’s hands extending and abducting the patient’s thumb and little finger ( long thin red arrows crossing over the patient’s thumb and little finger).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



