Tibial Tuberosity Fractures
Eric W. Edmonds
DEFINITION
Tibial tuberosity fractures are rare fractures that predominately occur in adolescents with the onset of proximal tibial physeal closure.
These apophyseal fractures occur almost exclusively in boys, but there are a few cases reported in girls.
Most commonly, the injury occurs at the initiation of a jump.
The association with prior tibial tuberosity traction apophysitis (Osgood-Schlatter syndrome) is possible but not always present.
ANATOMY
The tibial tubercle exists in an anterolateral location on the proximal tibia just distal to the physis and develops in four recognized stages5 that are important to understanding potential pathology.14
Stage 1: The tubercle is completely a cartilage anlage without a secondary center of ossification.
Stage 2: known as the apophyseal stage, occurs between ages 8 and 12 years in girls and 9 and 14 years in boys. The secondary center of ossification is present but not contiguous with the epiphyseal ossification of the proximal tibia.
Stage 3: known as the epiphyseal stage, occurs when the apophyseal ossification connects with the epiphyseal bone; commonly occurring between ages 10 and 15 years for girls and 11 and 17 years for boys
Stage 4: is identified by complete fusion of the tubercle and closure of the apophyseal cartilage
Closure of the proximal tibial physis and the tubercle apophysis occurs in a predictable pattern.14 The proximal tibial physis closes in a posteromedial to anterolateral direction toward the tubercle apophysis, which is simultaneously closing in a proximal to distal direction.
The patellar ligament (tendon) inserts into the apophysis with a large periosteal insertion distally.
It is important to remember the native anterolateral position of the tubercle and therefore the fracture fragment when preoperatively planning the approach for intra-articular visualization.
The anterior tibial recurrent artery is at risk to rupture with a displaced fracture. Bleeding from its proximal branches as it retracts into the anterolateral compartment could cause a compartment syndrome.
PATHOGENESIS
The injury occurs with a forceful quadriceps contraction while the foot is fixed. There is a significant eccentric force of the quadriceps mechanism that overcomes the strength of the apophysis and the surrounding periosteum.10 A second possible mechanism of injury is sudden passive knee flexion while the quadriceps is contracted.
It has been hypothesized that individuals with this fracture may have quadriceps strength that is greater than their peers.8 Thus, the conditions for the fracture are present during jumping and in strong individuals.
The injury usually occurs at a time when the tuberosity is undergoing normal closure,14 and the pattern of normal skeletal maturity results in specific fracture patterns.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients usually present acutely with significant pain and an inability to bear weight on the affected leg after sustaining an injury during physical activity. They are usually tender, with significant swelling over the anterior proximal tibia. An effusion may be present, and active straight-leg raise against gravity is often not possible.
Children with minimally displaced fractures may extend the knee but with obvious discomfort (likely due to intact retinaculum and surrounding periosteum).
Neurovascular examination should always be performed, as there is distinct risk of injury with tibia tubercle fractures.
There should also be an evaluation for the presence of leg compartment syndrome.
Osgood-Schlatter syndrome has a more insidious onset and usually will not have an effusion or result in extensor lag, even though it may be significantly tender over the tubercle.
RADIOGRAPHIC FINDINGS
Good anteroposterior (AP) and lateral radiographs are often able to make the diagnosis, but they may be limited in the assessing the extent of injury.14
The displacement is most obvious on the lateral radiograph.
Lateral radiographs with about 15 degrees internal rotation can place the tubercle on profile and assist with the assessment of nondisplaced or minimally displaced fractures. Contralateral images can be helpful for comparison and may help confirm the diagnosis.
Ogden et al13 described three types of tubercle fractures using only the lateral x-ray:
Type I: fractures through the apophysis only
Type II: fractures that exit between the epiphysis and apophysis
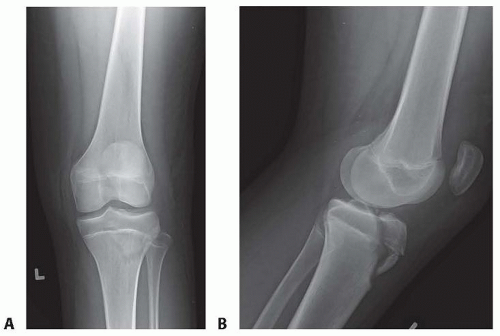
FIG 1 • AP (A) and lateral (B) radiographs of a 16-year-old boy who sustained a tibial tuberosity fracture. The fracture is a type III or type C, which enters the knee joint.
Type III: fractures that propagate into the anterior knee joint under the anterior meniscus attachments (FIG 1)
A multiplanar imaging classification scheme has also been described that takes the skeletal development and risk for associated injuries into consideration.14Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



