The Practical Exam in Electromyography
Ernest W. Johnson
William S. Pease
Each question refers to one figure. The figures are from Dr. Johnson’s well-known slide collection gathered over the years from a variety of EMG instrument displays. Depending on your experience this will represent either a history lesson in instrument displays or memories. Abbreviations are defined in the appendix. Answers and comments follow.
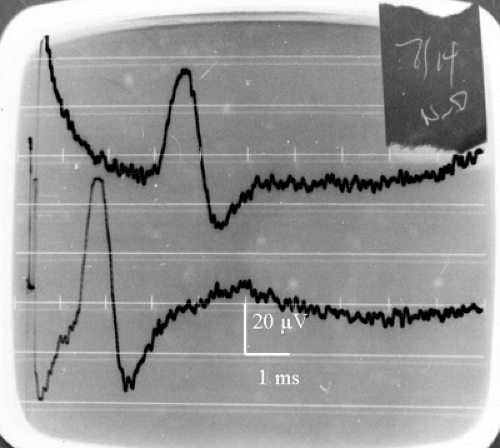 Top trace: digit 3, wrist stimulation at 14 cm Bottom trace: digit 3, midpalm stimulation at 7 cm |
1. What is your conclusion?
A. Carpal tunnel syndrome, mild
B. Normal
C. Cold hand
D. Technique error
View Answer
B Latencies and amplitutdes are normal for this technique. Amplitude change represents normal temporal dispersion. See Figure 8-19
 2. SNAP recorded from digit 1 Top trace: stimulate both median and radial nerves at wrist Middle trace: stimulate median nerve at wrist Bottom trace: stimulate radial nerve at wrist |
2. What is your diagnosis?
A. Normal
B. Carpal tunnel syndrome
C. Peripheral neuropathy, mild
D. Both B and C
View Answer
D Radial response has a mildly prolonged latency, with a long duration and low amplitude; this suggests axonal neuropathy. Additional delay in latency and reduction in amplitude of median response suggest carpal tunnel syndrome in the setting of a vulnerable nerve in the face of neuropathy. The ratio of median to radial SNAP amplitude is typically 2:1. See Figure 9-20. The two-humped recording (top) is termed the Bactrian sign.
 SNAP recorded from digit 1 (stimulate wrist 10 cm) Top trace: stimulate radial nerve at wrist 10 cm Bottom trace: stimulate median nerve at wrist |
3. What is your diagnosis?
A. Carpal tunnel syndrome, mild
B. Normal
C. Peripheral neuropathy, mild
D. Cold hand
View Answer
B The latencies of the responses are within 0.1 ms, and the median SNAP shows an amplitude four times that of the radial. Contrast with pathologic responses in question 2.
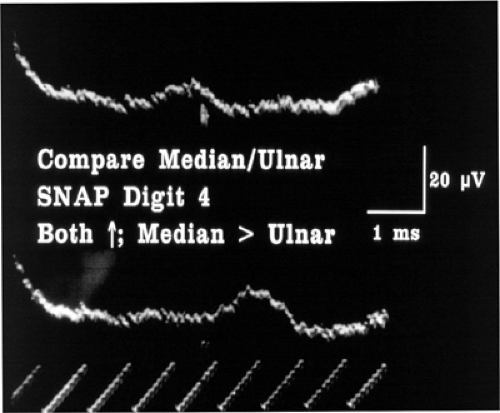 SNAPs recorded from digit 4 stimulate at wrist 14 cm Top trace: ulnar nerve Bottom trace: median nerve |
4. What is your diagnosis?
A. Carpal tunnel syndrome
B. Peripheral neuropathy, mild
C. Cold hand
D. Both A and B
View Answer
D Median latency is markedly prolonged at 6 ms, and ulnar latency is also prolonged at 4.5 ms. Small amplitudes of the responses argue against an error due to cold temperature. See Figure 8-21.
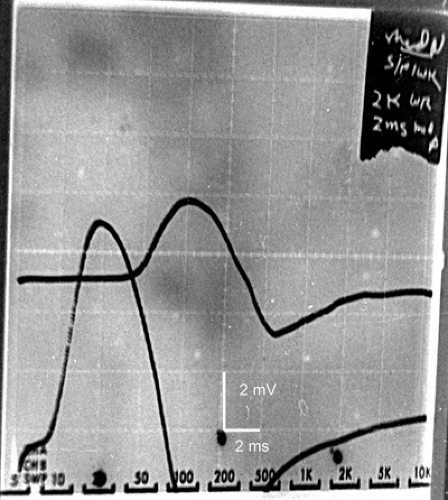 CMAP recorded from abductor pollicis brevis (thenar) Upper trace: stimulate wrist 8 cm Lower trace: stimulate at thenar crease |
5. What is your diagnosis?
A. Normal
B. Severe carpal tunnel syndrome
C. Mild carpal tunnel syndrome
D. Cold hand
View Answer
C Wrist latency recording is abnormal at 5 ms, with CMAP amplitude of only 3 mV. At first one might think this a severe carpal tunnel syndrome because of the small amplitude; however, the results of stimulation of the recurrent thenar branch in the palm demonstrate that there is conduction block, leading to a conclusion of mild carpal tunnel syndrome. The prognosis for nerve recovery is excellent in the situation of conduction block (neurapraxia). See Figure 9-10.
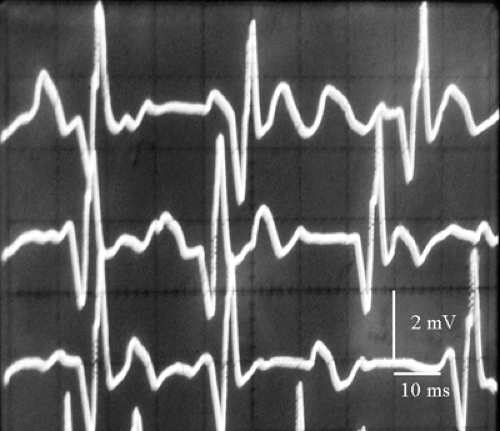 Needle in anterior tibialis muscle |
6. In which condition was this recorded?
A. Crossed leg palsy s/p 5 months
B. Prior poliomyelitis
C. Acute L5 radiculopathy
D. Amyotrophic lateral sclerosis
View Answer
C The rapid rate of motor unit potential (MUP) firing (30 Hz) suggests neuropathy. The MUP is within the normal range for amplitude, duration, and phases, and these measurements make it unlikely that the MUP was recorded from a chronic neuropathic condition.
 7. Which nerve is compromised? |
A. Anterior interosseus
B. Distal ulnar
C. Deep radial (post. interosseus)
D. Proximal radial
View Answer
C The classic “hook ’em horns” sign of posterior interosseus (deep radial) palsy is shown. All of the finger extensors are weak from the injury, but the force generated from both passive and active components of the extensor digiti minimi and the extensor indicis is combined with that of the extensor digitorum, resulting in slightly worse extension force in the middle and ring fingers.
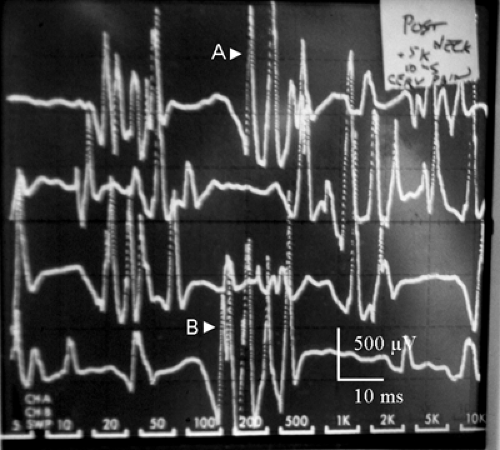 Consider the polyphasic MUP at B. |
8. Why does it have more phases than when it first appears at A?
A. Unstable MUP
B. Two overlapping MUPs
C. Artifact of concentric needle EMG recording
D. Repetitive activation of one MUP
View Answer
B Following the MUPs in time in these rastered traces demonstrates the individual potentials overlapping and interfering to varying degrees. Some of the potentials do appear polyphasic, and one cannot be sure of stability of the MUPs.
 Monopolar EMG needle in trapezius muscle
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
