Abstract
Purpose of the study
We performed an isokinetic analysis of both shoulders in 102 male patients suffering from shoulder instability after several trauma-related anterior or anterior-inferior dislocations. The analysis was part of a comprehensive medical and radiological assessment (with standard X-rays and cross-sectional imaging) prior to surgery. The study’s objective was to measure the strength of the patients’ internal and external rotators after recurrent dislocations (by comparing injured and healthy sides) and to evaluate the dislocations’ impact on the muscles on the injured side.
Materials and methods
The mean patient age was 24.8 (range: 16–47). We analysed the impact of instability on rotator muscle performance according to the side (dominant or non-dominant), the number of dislocations and the severity of any associated bone damage. The isokinetic analysis was performed at least one month after the last shoulder dislocation. The same operator performed all procedures. The modified Davies position was adopted, in order to record the peak torque of the internal and external rotators during concentric contractions at 60° and 180° per second. Means and standard deviations for peak torque to body weight ratios and external/internal rotator peak torque ratios were reported.
Results
After several anterior or anterior-inferior shoulder dislocations, there was a non-significant difference in the external rotator/internal rotator ratio when comparing injured and healthy sides – regardless of whether the injured side was dominant or not, the number of dislocations and the severity of bone damage.
Conclusion
Systematic, presurgical, isokinetic testing of the shoulder does not appear to be of value in post-traumatic instability in male patients.
Résumé
Nous avons effectué un bilan isocinétique systématique des deux épaules à 102 hommes, présentant tous une instabilité secondaire à plusieurs luxations antérieures ou antéro-inférieures d’origine traumatique. Ce test intervenait dans le bilan préopératoire qui comprenait un bilan clinique et radiologique (radiographies standards ± imagerie en coupe). Le but de cette étude était: d’évaluer la force musculaire des rotateurs internes et externes de l’épaule lésée et de comparer les résultats avec ceux obtenus du côté controlatéral sain ; d’étudier le retentissement de l’instabilité sur l’équilibre musculaire des rotateurs internes et externes de l’épaule lésée.
Population et méthode
L’étude a concernée 102 hommes, âge moyen 24,8 ans. Nous avons évalué le retentissement de l’instabilité sur l’équilibre des rotateurs en fonction du côté lésé : dominant ou non, du nombre d’épisodes d’instabilité, ainsi que de l’importance des lésions osseuse associées. Tous les tests ont été réalisés par le même opérateur, sur le même dynamomètre : Cybex Norm ; nous avons évaluer les rotateurs médiaux et latéraux ainsi que le rapport RL/RM en mode concentrique à 60° et 180°/s. Le délai entre le dernier épisode d’instabilité et le test était au minimum de un mois.
Résultats
On ne retrouve pas de différence significative des valeurs du rapport RL/RM en mode concentrique : quel que soit le côté lésé (dominant ou non), le nombre d’épisodes d’instabilité ou l’importance des lésions osseuses.
Conclusion
Il ne semble pas y avoir d’intérêt à inclure un test isocinétique systématique en préopératoire dans le cadre d’instabilité post-traumatique chez les hommes.
1
English version
1.1
Introduction
In 1890, Broca and Hartman hypothesized that recurrence after an initial traumatic anterior-inferior dislocation of the shoulder was related to the presence of damage to the glenoid labrum and a posterior defect of the head of the humerus. In 1950, De Palma criticized this hypothesis and suggested that recurrent glenohumeral instability was predominantly due to a neuromuscular imbalance caused by rotator muscle damage at the time of the initial trauma. Isokinetic evaluation is now acknowledged to be a reliable technique for evaluating the performance of the shoulder rotator muscles. It enables the detection of impairments in some muscle groups and the identification of disease-induced perturbations of the agonist-antagonist balance.
The objective of the present study was to:
- •
study the possible impact of post-traumatic instability on the muscle balance between the internal rotators (IRs) and external rotators (ERs) of the injured shoulder as a function of dominance, the number of dislocations and the severity of any associated bone damage;
- •
and specify the indication for isokinetic evaluation.
1.2
Materials and methods
We performed a prospective study between April 2004 and January 2009.
1.2.1
Population
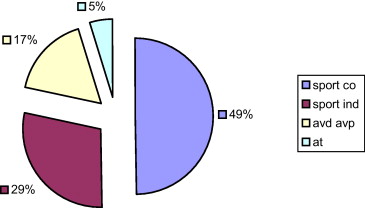
We performed a comprehensive, isokinetic assessment of both shoulders on 102 male patients, all of whom presented secondary instability following one or more anterior or anterior-inferior dislocations of traumatic origin. The mean patient age was 24.8 (range: 16–47) and the morphological characteristics of the study population are summarized in Table 1 . The causes of instability are detailed in Fig. 1 .
| Patients | Age (years) | Weight (Kg) | IMC | Number of recurrences |
|---|---|---|---|---|
| Dominant side injured ( n = 64) | 23 | 72.3 | 23.3 | 4 (2–10) |
| Non dominant side injured ( n = 38) | 26 | 73.5 | 23.7 | 4 (2–8) |
1.2.2
Inclusion criteria
All subjects had presented at least one documented episode of anterior or anterior-inferior post-traumatic dislocation. The mean number of instability episodes was 4 (range: 1–10).
The injured shoulder was on the dominant side in 64 subjects and on the non-dominant side in 38; there were no significant morphological differences between these two groups. Likewise, the mean number of instability episodes was similar in the two groups.
The time interval between the first traumatic dislocation and the isokinetic testing was 38 months, on average (range: 4–146). The isokinetic testing was always carried out at least one month after the last instability episode (range: 1–6).
Most patients had received orthopaedic and rehabilitation care following the initial dislocation, with the elbow immobilized against the body for between 8 and 20 days. The rehabilitation typically combined strengthening of the IRs with proprioceptive work.
The recurrences had not always been followed by rehabilitation. All patients were assessed with standard X-rays and cross-sectional imaging. Ninety-eight subjects had undergone arthrography and four had undergone magnetic resonance imaging.
1.2.3
Exclusion criteria
Subjects presenting episodes of non-traumatic instability or associated damage (such as rupture of the rotator cuff or fracture of the humerus) were excluded from the study.
1.2.4
Isokinetic testing
Isokinetic testing was always performed as part of a presurgical assessment. All tests were performed by the same operators in the Department of Sports Medicine at Rennes University Hospital and were always preceded by a clinical examination to check for the absence of contraindications (pain, limited joint movement, etc.).
Each patient received a study information sheet describing the test and the possible complications.
All tests were performed on the same Cybex Norm dynamometer. The subject adopted the modified Davis position, i.e. a sitting position with the arm held at an angle of between 25° and 45° in the plane of the scapula and with the elbow flexed at angle of 90°.
1.2.5
Order of test performance
The injured side was always tested first, in order to determine the maximum pain-free joint amplitudes. We rigorously noted the positional parameters, so that identical joint amplitudes were tested on each side.
Measurements were performed after the patient had warmed up on the dynamometer; the length of the warm-up was not set in advance, so that the subject could familiarize himself with the procedure and, above all, felt confident about performing the test.
The test always started with the arm in external rotation. The patient performed three repetitions at a low angular velocity (60°/s). Then, after a 20-second rest, the patient performed five repetitions at high velocity (180°/s). We recorded the concentric-mode peak torque (relative to bodyweight, i.e. in Nm/kg) for the IRs and ERs at both velocities and also calculated the ER/IR ratio.
1.2.6
Statistical analysis
The study endpoints were the peak torque (relative to bodyweight; expressed in Nm/kg) for the IRs and ERs and the ER/IR ratio at both velocities (60°/s and 180°/s).
In each group, we compared the values recorded on the healthy and injured sides. Wilcoxon’s non-parametric test for matched samples (a signed rank test) was applied with BiostaTGV software ( http://marne.u707.jussieu.fr/biostatgv/ ). Application of this statistical test meant that we did not have to check the distribution and variance in each group.
The threshold for statistical significance was set to P < 0.05.
1.3
Results
1.3.1
Overall results (102 subjects)
There were no significant differences between the injured and healthy sides in terms of IR or ER strength or the ER/IR ratio ( Table 2 ).
| Peak torque (Nm) % bodyweight | Overall results n = 102 | Dominant side injured n = 64 | Non-dominant side injured n = 38 | |||
|---|---|---|---|---|---|---|
| Healthy side | Injured side | Healthy side | Injured side | Healthy side | Injured side | |
| RM 60°/s | 0.72 (0.12) | 0.71 (0.12) NS | 0.72 (0.12) | 0.74 (0.12) NS | 0.73 (0.12) | 0.68 (0.11) P = 0.06 |
| RL 60°/s | 0.32 (0.08) | 0.31 (0.07) NS | 0.32 (0.07) | 0.31 (0.07) NS | 0.34 (0.08) | 0.30 (0.08) P = 0.04 |
| RL/RM 60°/s | 0.45 (0.09) | 0.43 (0.09) NS | 0.44 (0.08) | 0.43 (0.08) NS | 0.45 (0.11) | 0.44 (0.09) NS |
| RM 180°/s | 0.59 (0.12) | 0.55 (0.14) P = 0.06 | 0.59 (0.13) | 0.58 (0.14) NS | 0.58 (0.11) | 0.52 (0.13) P = 0.04 |
| RL 180°/s | 0.25 (0.06) | 0.23 (0.06) NS | 0.24 (0.06) | 0.24 (0.05) NS | 0.26 (0.07) | 0.23 (0.06) NS |
| RL/RM 180°/s | 0.43 (0.09) | 0.44 (0.11) NS | 0.42 (0.09) | 0.43 (0.11) NS | 0.44 (0.09) | 0.45 (0.11) NS |
1.3.2
The influence of dominance
1.3.2.1
Injury to the dominant-side injury (64 subjects)
There were no significant differences between the injured and healthy sides in terms of IR or ER strength or the ER/IR ratio ( Table 2 ).
1.3.2.2
Injury to the non-dominant side (38 subjects)
There was no significant difference in the ER/IR ratio when comparing the injured and healthy sides ( Table 2 ). We observed a general trend towards muscle weakness on the injured, non-dominant side, relative to the healthy, dominant side. There was a significant difference for the ERs at 60°/s and the IRs at 180°/s The values were slightly lower on the non-dominant side but (when considering the results in the previous section) appeared to be more related to non-dominance than to injury.
1.3.3
The influence of the number of recurrences
1.3.3.1
One or two recurrences (42 subjects)
There was no significant difference in the ER/IR ratio when comparing the injured and healthy sides ( Table 3 ). There was a general trend towards weakness of the IRs and ERs on the injured side, at both velocities.
| Peak torque (Nm) % bodyweight | Number of recurrences < 3 n = 42 | Number of recurrences 3 to 5 n = 38 | Number of recurrences > 5 n = 22 | |||
|---|---|---|---|---|---|---|
| Healthy side | Injured side | Healthy side | Injured side | Healthy side | Injured side | |
| RM 60°/s | 0.74 (0.11) | 0.72 (0.12) NS | 0.72 (0.13) | 0.72 (0.13) NS | 0.70 (0.11) | 0.70 (0.11) NS |
| RL 60°/s | 0.32 (0.07) | 0.31 (0.08) NS | 0.33 (0.07) | 0.31 (0.07) P = 0.03 | 0.32 (0.09) | 0.30 (0.06) NS |
| RL/RM 60°/s | 0.44 (0.08) | 0.43 (0.1) NS | 0.46 (0.09) | 0.43 (0.08) NS | 0.46 (0.12) | 0.43 (0.07) NS |
| RM 180°/s | 0.61 (0.12) | 0.58 (0.13) P = 0.02 | 0.58 (0.13) | 0.54 (0.16) P = 0.01 | 0.56 (0.12) | 0.54 (0.13) NS |
| RL 180°/s | 0.25 (0.05) | 0.24 (0.06) NS | 0.25 (0.07) | 0.23 (0.06) NS | 0.25 (0.07) | 0.23 (0.04) NS |
| RL/RM 180°/s | 0.41 (0.09) | 0.42 (0.09) NS | 0.43 (0.09) | 0.45 (0.11) NS | 0.45 (0.11) | 0.45 (0.13) NS |
1.3.3.2
Three to five recurrences (38 subjects)
There was no significant difference in the ER/IR ratio when comparing the injured and healthy sides ( Table 3 ). There was a general trend towards weakness of the IRs and ERs on the injured side, at both velocities.
1.3.3.3
More than five recurrences (22 subjects)
The peak torque for the IRs was similar at 60°/s and lower at 180°/s when comparing the injured and healthy sides ( Table 3 ).
The peak torque for the ERs was lower at both velocities on the injured side.
The ER/IR ratio was lower at 60°/sec but did not differ significantly, there was no difference at 180°/s when comparing the injured and healthy sides.
Overall (and regardless of the number of instability episodes), we observed a general trend towards weakness of the rotators on the injured side but did not see a significant difference in the ER/IR torque ratio measured in concentric mode.
1.3.4
The influence of bone damage
1.3.4.1
Presence of posterior, notch-like damage to the head of the humerus (35 subjects)
There was no significant difference in the ER/IR ratio when comparing the injured and healthy sides ( Table 4 ). We observed a general trend towards weakness of the IRs and ERs on the injured side and at both velocities. The weakness was significant for the IRs at 180°/s.
| Peak torque (Nm) % bodyweight | Notch-like damage n = 35 | Damage to the lower glenoid cavity n = 21 | Notch-like damage + Damage to the lower glenoid cavity n = 8 | |||
|---|---|---|---|---|---|---|
| Healthy side | Injured side | Healthy side | Injured side | Healthy side | Injured side | |
| RM 60°/s | 0.75 (0.11) | 0.73 (0.12) NS | 0.72 (0.1) | 0.72 (0.12) NS | 0.77 (0.19) | 0.76 (0.14) NS |
| RL 60°/s | 0.32 (0.07) | 0.30 (0.07) NS | 0.32 (0.08) | 0.30 (0.08) NS | 0.35 (0.05) | 0.32 (0.07) NS |
| RL/RM 60°/s | 0.44 (0.09) | 0.42 (0.09) NS | 0.44 (0.09) | 0.42 (0.07) NS | 0.47 (0.07) | 0.42 (0.1) NS |
| RM 180°/s | 0.60 (0.11) | 0.57 (0.14) P = 0.009 | 0.59 (0.12) | 0.55 (0.16) NS | 0.59 (0.17) | 0.57 (0.17) NS |
| RL 180°/s | 0.24 (0.06) | 0.23 (0.05) NS | 0.25 (0.06) | 0.24 (0.06) NS | 0.28 (0.07) | 0.25 (0.05) NS |
| RL/RM 180°/s | 0.41 (0.1) | 0.42 (0.11) NS | 0.43 (0.1) | 0.45 (0.14) NS | 0.47 (0.09) | 0.44 (0.09) NS |
1.3.4.2
Presence of damage to the lower glenoid cavity (21 subjects)
There was no significant difference in the ER/IR ratio when comparing the injured and healthy sides ( Table 4 ). We observed a general trend towards weakness of the IRs and ERs on the injured side and at both velocities.
1.3.4.3
Presence of damage to the lower glenoid cavity and posterior, notch-like damage to the head of the humerus (eight subjects)
There was no significant difference in the ER/IR ratio when comparing the injured and healthy sides ( Table 4 ). We observed a general trend towards weakness of the IRs and ERs and low ER/IR ratios on the injured side and at both velocities.
Overall, and regardless of the type of bone damage, we did not observe any significant differences in ER/IR ratios measured in concentric mode.
1.4
Discussion
The objective of the present work was to study the possible impact of recurrences of post-traumatic anterior and anterior-inferior dislocations on the shoulder IR/ER muscle balance.
Our study concerned only male patients; this type of recruitment was prompted by literature data showing that post-traumatic dislocations are more frequent in men. Zachilli and Owens found that males accounted for 71.8% of the patients attending the emergency room for this condition (with an annual incidence of 23.9 per 100,000 subjects).
The mean patient age in our study was 24.8 (range: 14–47), which is similar to that generally found by other authors. Zachilli and Owens observed that 46.8% of trauma incidents concerned the 15–29-age class. Owens et al. reported an annual incidence of 169 per 100,000 subjects for US military personnel and 435 per 100,000 subjects for military cadets.
Sport was the most frequent cause of dislocation and accounted for 78% of the cases in our study ( Fig. 1 ); this value was 48% for Zacchilli and Owens , 47% for Simonet et al. and 96% for Owens et al. . These differences can be explained by the nature of the patient recruitment: the values reported by Zacchilli and Owens and Simonet et al. corresponded to emergency room admissions, whereas Owens’ et al. study was performed in military academies. In our present study, many of the subjects were students and played sport (kayaking, judo, handball, soccer, etc.) on a regular basis; indeed, a good proportion were high-level sportsmen in regional and national squads.
The management of shoulder instability has been addressed by many authors . Hovelius et al. estimated that half of the subjects aged 12 to 25 undergoing rehabilitation after a first episode of instability did not suffer from recurrence and that compliance with post-traumatic immobilization did not appear to influence the risk of recurrence. In contrast, Itoi et al. recommended immobilization in an external rotation brace, which appeared to be associated with a decreased risk of recurrence. However, Finestone et al. did not find a significant relationship between internal or external immobilisation and the rate of recurrence after initial dislocation. In a study with 7 years of follow-up of anterior glenohumeral dislocations, Tsai et al. noted that 65% of the subjects reported instability during physical activity.
In fact, it appears that age, side (dominant vs. non-dominant), gender, the severity of initial bone damage (a posterior chip fracture or damage to the lower edge of the glenoid cavity) and the level and type of sport are more important predictive factors than immobilization in the risk of recurrence . These various criteria were met in our present study: the population was young (mean age: 24.8), with a high proportion of keen sportsmen; the trauma was on the dominant side in 63% of cases and was associated with a posterior chip fracture of the humeral head in 33% of cases, damage to the lower edge of the glenoid cavity in 20% of cases and both types of damage in under 10% of cases.
Although isokinetic testing of the shoulder has been extensively studied , there are still a number of disparities in terms of the body positions, velocities and protocols used. However, there appears to be a consensus in favour of the Davis modified position as the reference position for the evaluation of painful and/or unstable shoulders. The supine position with the arm abducted at 90° is used above all when evaluating throwers and in the absence of an underlying pathology.
Concentric mode measurements are reproducible, as long as the protocol is rigorously adhered to . In our study, we used the modified Davis position. We always tested the injured shoulder first, while limiting the movement to pain-free amplitudes and allowing the subject to warm up for as long as required (in order to dispel any apprehension). We performed all our measurements in a concentric mode, in order to maximize reproducibility and decrease the risk of injury.
Many studies have tried to establish reference values for isokinetic measurements of rotator muscles in the healthy shoulder. Different parameters influence the outcome of these measurements, such as age, gender, the subject’s morphology, dominance vs. non-dominance, the type of sporting activity, the subject’s occupation, the dynamometer used for the tests, the angular velocities and the subject’s position during the test.
In sedentary subjects, one does not observe a significant difference between the dominant and non-dominant arms. In contrast, higher IR torque values are found for the dominant arm in sportspeople practicing asymmetric sports, such as tennis , baseball and volleyball . Consequently, ER/IR ratios are lower. Some authors consider that imbalance may cause the shoulder pain frequently experienced in these groups of sportspeople .
Research on imbalance of the shoulder IRs and ERs in the aftermath of dislocation has yielded contradictory results; some authors consider that instability is favoured by an impairment of the IRs, whereas others believe that impairment of the ERs is to blame . These studies concerned small, heterogeneous populations (a mixture of males and females, sportspeople and sedentary subjects, etc.) in whom glenohumeral instability was not always due to trauma. Our study solely concerned men presenting with post-traumatic anterior or anterior-inferior instabilities. In this well-defined setting, we did not find any significant difference in the ER/IR ratios (measured in concentric mode) when comparing the healthy side and the injured side, regardless of whether the injured shoulder was dominant or not, the number of dislocations and the severity of bone damage observed.
We consider that isokinetic testing is of value in cases in which the traumatic origin of the instability is uncertain and radiographic screening is negative. In these cases, the discovery of muscle imbalance would guide the physician’s choice of a rehabilitation programme. In contrast, a confirmed lack of muscle imbalance would provide an additional argument in favour of joint injury and would prompt the physician to perform additional radiological screening for labral damage.
1.5
Conclusion
In the present study population, post-traumatic dislocations had no impact on the muscle balance of the shoulder rotators (as measured in concentric isokinetic mode).
These observations validate Broca and Hartman’s hypothesis in a post-traumatic setting, whereas the theory of “muscle imbalance” developed by De Palma appears to apply only to non-traumatic instabilities.
These observations prompt us to question the usefulness of rehabilitation (and notably specific strengthening of the IRs) after an episode of post-traumatic instability, as is generally recommended. Indeed, our findings raise the question of whether proprioceptive work alone might be sufficient.
In any case, we consider that concentric-mode, isokinetic testing is not essential in patients with post-traumatic anterior or anterior-inferior dislocations.
Disclosure of interest
The authors declare that they have no conflicts of interest concerning this article.
Related posts:
 Psychotherapeutic follow up of out patients with traumatic brain injury: Preliminary results of an individual neurosystemic approach
Psychotherapeutic follow up of out patients with traumatic brain injury: Preliminary results of an individual neurosystemic approach
 Effects of a home-based rehabilitation program in obese type 2 diabetics
Effects of a home-based rehabilitation program in obese type 2 diabetics
 Translation in Arabic, adaptation and validation of the SF-36 Health Survey for use in Tunisia
Translation in Arabic, adaptation and validation of the SF-36 Health Survey for use in Tunisia
 Physical and rehabilitation medicine (PRM) care pathways: “Spinal cord injury”
Motor system after neonatal arterial ischemic stroke: MRI studies
Physical and rehabilitation medicine (PRM) care pathways: “Spinal cord injury”
Motor system after neonatal arterial ischemic stroke: MRI studies
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


