The Head and Neck
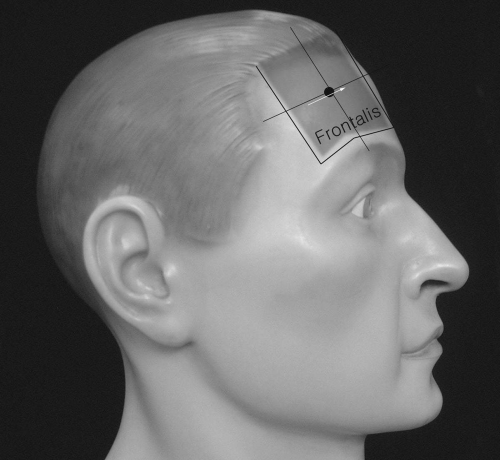
Frontalis
Patient Position:
Supine with head slightly turned (tilted) to the opposite side.
Needle Insertion:
The muscle is flat and extremely thin. Insert a short and small needle into the muscle at a 10- to 20-degree angle to the skin (relatively sharp angle) approximately at the midline between the front hair line and the eyebrow.
Activation:
Ask the patient to raise the eyebrows or wrinkle the forehead.
Clinical Notes:
Normal motor unit action potential amplitude and duration in this muscle are usually small and short. It is often difficult to differentiate from fibrillation potentials. It also fires rapidly.
Innervation:
Facial nerve (C VII).
Orbicularis Oculi
Patient Position:
Supine with head slightly tilted to the opposite side.
Needle Insertion:
Before inserting the needle, make sure of the orbital fossa and its lateral, upper, and inferior borders. Insert the needle at about 1.5 centimeters (cm) from the lateral bony margin of the orbital fossa and direct it upward or downward obliquely. Insert and advance the needle at a relatively sharp angle because the muscle layer is extremely thin and superficial.
Activation:
Close eyelids.
Clinical Notes:
Important muscle from a cosmetic (facial expression) and functional (eye closure) standpoint after facial paralysis. Black and blue markings may result from needling. A firm compression with dry cotton or gauze may be necessary after the needle is removed.
Innervation:
Facial nerve (C VII).
Origin:
Nasal part of the frontal bone, frontal process of the maxilla, and anterior surface of the medial palpebral ligament.
Insertion:
Muscle fibers surround the circumference of the orbit, spread downward on the check, and blend with adjacent structures.
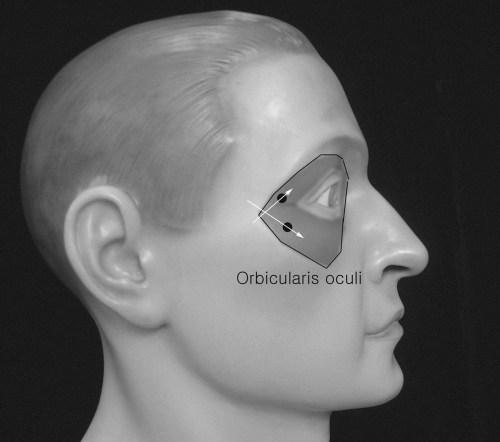 Figure 21-2. Orbicularis oculi. |
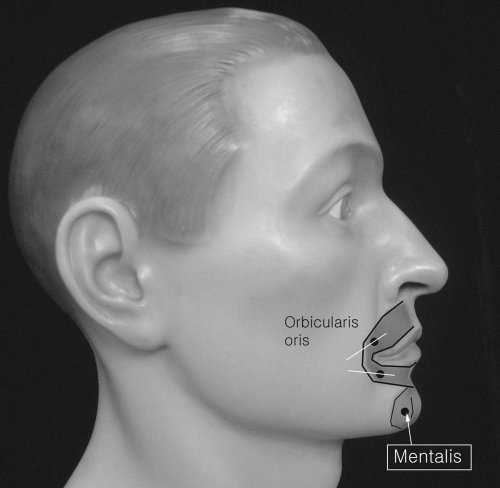
Orbicularis Oris
Patient Position:
Supine with the head slightly tilted to the opposite side.
Needle Insertion:
Insert the needle 0.5 to 1 cm below or above the mouth angle and gradually advance it toward the midline while having the patient pucker his/her lips.
Activation:
Ask the patient to whistle or pucker the lips.
Clinical Notes:
Rare, but isolated neuropathy of superior or inferior bucccal branches of facial nerve may be seen. Therefore, both upper and lower parts of this muscle may need to be tested separately.
Innervation:
Facial nerve (C VII).
Origin:
Numerous strata of muscle fibers surrounding the orifice of the mouth, derived in part from other facial muscles.
Nasalis
Patient Position:
Supine and head tilted slightly to the opposite side.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


