Abstract
There are two main surgical treatments for osteoarthritis: conservative treatments, where the damaged cartilage is left in place, and radical treatments, where the cartilage is replaced by an artificial endoprosthesis; this latter procedure is termed joint arthroplasty. These treatments are only offered to symptomatic patients. Arthrodesis is yet another surgical intervention in cases of osteoarthritis. It will sacrifice the joint’s articular function and is performed on small osteoarthritic joints, such as wrists and ankles, for instance. Osteoarthritis symptoms are usually the consequence of an imbalance between the load applied to a joint and the surface available to support that load. Therefore, conservative treatments will either tend to decrease the load exerted on the joint, such as in a tibial valgus osteotomy for instance, or to improve the articular surface supporting that load. Sometimes, both can be provided at the same time; the peri-acetabular osteotomy for hip dysplasia is an example of such a procedure. Conservative treatments are usually offered to young patients in order to delay, if not avoid, the need for a joint prosthesis. They are usually performed before osteoarthritis appears or at an early stage. Joint arthroplasties have overwhelmingly excellent functional results and today’s research is directed towards providing rapid recovery, very long-term stability, and the assurance of a good functionality in extreme conditions. However, complications with joint arthroplasties can be serious with little, if any, reasonable salvage solution. Therefore, these procedures are offered to patients who have failed adequate medical treatment measures.
1
Introduction
There are two main surgical treatments for osteoarthritis (OA): conservative, with the damaged cartilage left in place, and radical, with the cartilage replaced by an artificial endoprosthesis, the latter procedure termed joint arthroplasty. These treatments are offered only to symptomatic patients. Arthrodesis is another surgical intervention in cases of OA. It sacrifices the joint’s articular function and is performed on small osteoarthritic joints, such as wrists and ankles.
OA symptoms usually result from an imbalance between the load applied to a joint and the surface available to support that load. Therefore, conservative treatments will tend to decrease the load exerted on the joint, such as in tibial valgus osteotomy, or improve the articular surface supporting that load. Sometimes, both solutions can be provided at the same time; peri-acetabular osteotomy for hip dysplasia is one example.
Conservative treatments are usually offered to young patients so as to delay, if not avoid, the need for joint prosthesis. They are usually performed before OA appears or at an early stage. Joint arthroplasty has overwhelmingly excellent functional results and today’s research is directed toward providing rapid recovery, very long-term stability, and the assurance of good functionality in extreme conditions. However, complications with joint arthroplasty can be serious with little, if any, reasonable salvage solution. Therefore, these procedures are offered to patients with failure of adequate medical treatment measures.
In the following sections, we discuss the main surgical treatments for hip, knee, and shoulder OA. We present both conservative and radical options along with patient selection criteria, a brief description of the technique, and the expected results.
2
Hip OA
2.1
Conservative treatment
Conservative surgical treatments of hip OA have declined over the last decades after the implementation of total hip replacement (THR). Nonetheless, significant indications remain for young patients. These treatments will surely delay but not always avoid the need for joint replacement in the long-term . The 3 main surgical procedures that can be performed are femoral osteotomy, pelvic osteotomy, and cartilage and labrum procedures under arthroscopy.
2.2
Femoral osteotomy
This osteotomy reorients the femoral head, with one of 2 main goals: positioning an adequate portion of the femoral cartilage in front of the acetabulum, such as in rotational osteotomy of the femoral neck for osteonecrosis , and changing the biomechanics of the hip to reduce the load going through the joint, such as in femoral varus osteotomy. The most common osteotomies are valgus and varus femoral osteotomies; others such as flexion, extension or rotation osteotomy or a combination of these are less frequent. The varus femoral osteotomy is usually indicated for hip dysplasia, osteonecrosis, and valgus deformation. It closes the neck-shaft angle when it is superior to 135° . The long-term results for early OA are good, with 75% 10-year survival, defined as the delay before hip replacement. Second-line hip replacement will have the same prognosis as first-line replacement. The procedure is not recommended with isolated serious dysplasia . Valgus femoral osteotomy is mainly performed for femoral neck non-union, slip upper-femoral epiphysis sequelae and congenital varus deformity of the femoral neck.
2.3
Pelvic osteotomy
Pelvis osteotomy (including the shelf procedure) is only rarely performed today but can still provide excellent results. The common eligibility criterion is a painful, dysplastic hip in a relatively young patient (usually < 30 years old). Beyond that, we also rely on some other indications such as cartilage degeneration stage and coxometric parameters to decide on the surgical procedure. Shelf operation consists of a bone graft addition on top of the hip where the femoral head is uncovered; although it provides support and balances the load, it does not provide cartilage ( Fig. 1 ).
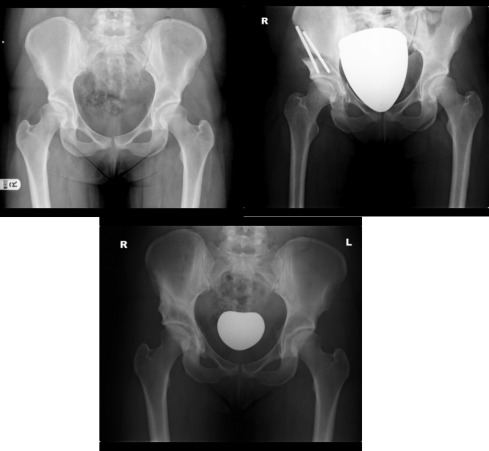
The Chiari osteotomy is an augmentation osteotomy similar to the shelf procedure that decreases the contact stresses going through the joint, even though it does not provide any cartilage. The Bernese peri-acetabular osteotomy is a reorientation procedure that lets the acetabulum rotate around the femoral head to cover the uncovered anterior and lateral portion of the head. .
When these surgeries are performed in carefully selected patients, they provide good results and delay the need for a hip replacement in the long-term. Conversion to hip replacement occurs at 10 years in about 40% of patients for the shelf procedure and in 15 to 20% for peri-acetabular and Chiari osteotomies. .
2.4
Arthroscopy
Arthroscopy is indicated for femoroacetabular impingement (FAI). It occurs when anatomic variation of the hip causes impingement between the femoral head–neck junction and the acetabular rim during functional motion. This condition is mainly seen in young and active men. Open or arthroscopic osteochondroplasty of the femoral head–neck junction is the surgical treatment for symptomatic cam impingement. Depending on the surgeon, it may be performed with an anterior open approach with or without arthroscopy by surgical dislocation or by arthroscopy exclusively. Good to excellent results are reported in 70 to 95% of patients.
2.5
THR
THR has been coined the “operation of the century”. Millions of THRs are performed worldwide to treat OA, with more than 95% of patients entirely satisfied with the functional results . The modern hip replacement was developed by Sir John Charnley in the 1960s and still represents the gold standard . However, significant improvements have been made over the last 50 years. The operation is performed now through a 6- to 8-cm incision and the patient stays about 3 nights in hospital, and just a few days after the surgery, can expect to walk normally with no walking aids and have a painless joint. Patients should not require revision for the next decades, if ever, and are free to return to complete activity including sports. There are few technical considerations, which we briefly discuss.
2.6
Bearing surfaces
The hip joint replacement is a ball-and-socket joint: it has a femoral head; the ball articulates the socket by a cup in the acetabulum. The materials in contact with each other are called bearing surfaces. Bearing surfaces are prone to wear, which may generate particulate debris and cause bone resorption and implant failure over time. Metal on polyethylene remains the most favored material among surgeons. It is cheap and easily machined in sizes and shapes. The latest developments such as highly crosslinked polyethylene have greatly decreased wear rates and almost obliterated the risk of particulate-induced osteolysis . Other bearings exist. Ceramic-on-ceramic bearings have been developed to avoid the wear problems with polyethylene. Indeed, there is no clinically measurable wear with this bearing. Nevertheless, this material has a risk of fracture < 1% . Metal-on-metal bearings are seldom used today because of the additional risks of adverse reaction to metal debris and metal ion in blood circulation and renal excretion.
2.7
Cemented and uncemented fixation
Two fixation methods exist, cemented and uncemented. Both are applicable to femoral stem and acetabular component. The results are similar and the preference for one or the other is mainly due to the surgeon or centre. In older patients, cemented fixation should be preferred because of the risk of fracture or non-integration of uncemented implants .
2.8
THR indications
THR is indicated with end-stage hip arthritis, when medical treatment has become ineffective, after an observation period of several weeks to several months. The excellent results of this procedure have widened its indications. Initially used exclusively with arthritis, it is today used in multiple situations such as osteonecrosis, secondary degenerative joint disease, congenital dislocation, hip fusion, bone tumor, hereditary disorders, and fractures of the femoral neck.
2.9
THR techniques
The surgery can be performed with various approaches. Each approach has relative advantages and drawbacks. The choice depends on the surgeon’s experience and choice and sometimes the anatomical characteristics of the patient. Recently, mini-invasive surgery (MIS) has permitted rapid recovery after the procedure. MIS decreases soft-tissue trauma, while allowing for adequate positioning of the prosthetic components. It contributes to dynamic stabilization of the hip . Some patients present complex hip cases such as developmental dysplasia of the hip, post-traumatic arthritis, or Legg-Calve-Perthes disease sequelae. In these cases, surgical techniques are more elaborate, and custom-made femoral implants may be necessary ( Fig. 2 ).

2.10
THR results
The clinical outcomes after THR are excellent . Rehabilitation after hospitalization is rarely needed, and only some patients will benefit from an additional period at a rehabilitation center before returning to independent living. Ambulatory surgery is possible for selected patients: those aged 40 to 75 years, with primary total hip arthroplasty and no history of myocardial infarction, pulmonary embolism, or anticoagulation therapy, no obesity and no important medical comorbidities. For these patients, in the Berger study, the mean time to resuming all activities of daily living was 10 days, and the mean time to walk 1/2 mile was 16 days . After 3 months, patients have no limitations in everyday life activities or sports. Charnley low-friction arthroplasty remains the gold standard with the longest follow-up. Long-term results are excellent, with only 23% revision at 25 years . Regarding more recent implants, mid-term results are equivalent to ceramic-on-ceramic replacements . Complications are unusual after THR. The most common are infection, dislocation and deep vein thrombosis and pulmonary embolism. The incidence of sepsis is 1%, on average, but is higher in patients with diabetes, rheumatoid arthritis, psoriasis, or sickle cell disease and a longer operation time . Improvement in surgical techniques and implant designs has greatly reduced the rate of dislocation, from 4% with a posterior approach in the 1990s to 0.5% with an anterior approach and modern implants currently . However, the risk of dislocation is increased in some cases such as with muscle weakness or neurological diseases, component malposition, bony impingement or previous hip surgery. Dual mobility sockets, which associates a small inner bipolar bearing that articulates with an outer true liner, are useful in reducing the risk of dislocation for these patients . Deep vein thrombosis and symptomatic pulmonary embolism are rare events, about 1%, with the current prophylaxis.
2.11
THR evolution
With the improvement in surgical techniques and perioperative care , recovery has improved vastly over the last decade and patients usually stay in the hospital for only 2 or 3 days. However, rehabilitation programs are beneficial for some patients such as very old patients and those with neurological deficiencies . However, initiatives are being developed to shorten the recovery period and hospital stay for relatively young patients without significant morbidity . Furthermore, with the improvement in implants, we expect the revision rate to decrease. The use of computer navigation for hip arthroplasty has increased over the last decade. Studies demonstrate substantial improvement in the accuracy of component positioning with navigation as compared with freehand alignment methods . However, the benefits of this additional surgical precision has yet to translate into improved long-term clinical outcomes . Resurfacing prostheses have not fulfilled their expectations and their advantages remain to be seen.
2
Hip OA
2.1
Conservative treatment
Conservative surgical treatments of hip OA have declined over the last decades after the implementation of total hip replacement (THR). Nonetheless, significant indications remain for young patients. These treatments will surely delay but not always avoid the need for joint replacement in the long-term . The 3 main surgical procedures that can be performed are femoral osteotomy, pelvic osteotomy, and cartilage and labrum procedures under arthroscopy.
2.2
Femoral osteotomy
This osteotomy reorients the femoral head, with one of 2 main goals: positioning an adequate portion of the femoral cartilage in front of the acetabulum, such as in rotational osteotomy of the femoral neck for osteonecrosis , and changing the biomechanics of the hip to reduce the load going through the joint, such as in femoral varus osteotomy. The most common osteotomies are valgus and varus femoral osteotomies; others such as flexion, extension or rotation osteotomy or a combination of these are less frequent. The varus femoral osteotomy is usually indicated for hip dysplasia, osteonecrosis, and valgus deformation. It closes the neck-shaft angle when it is superior to 135° . The long-term results for early OA are good, with 75% 10-year survival, defined as the delay before hip replacement. Second-line hip replacement will have the same prognosis as first-line replacement. The procedure is not recommended with isolated serious dysplasia . Valgus femoral osteotomy is mainly performed for femoral neck non-union, slip upper-femoral epiphysis sequelae and congenital varus deformity of the femoral neck.
2.3
Pelvic osteotomy
Pelvis osteotomy (including the shelf procedure) is only rarely performed today but can still provide excellent results. The common eligibility criterion is a painful, dysplastic hip in a relatively young patient (usually < 30 years old). Beyond that, we also rely on some other indications such as cartilage degeneration stage and coxometric parameters to decide on the surgical procedure. Shelf operation consists of a bone graft addition on top of the hip where the femoral head is uncovered; although it provides support and balances the load, it does not provide cartilage ( Fig. 1 ).

The Chiari osteotomy is an augmentation osteotomy similar to the shelf procedure that decreases the contact stresses going through the joint, even though it does not provide any cartilage. The Bernese peri-acetabular osteotomy is a reorientation procedure that lets the acetabulum rotate around the femoral head to cover the uncovered anterior and lateral portion of the head. .
When these surgeries are performed in carefully selected patients, they provide good results and delay the need for a hip replacement in the long-term. Conversion to hip replacement occurs at 10 years in about 40% of patients for the shelf procedure and in 15 to 20% for peri-acetabular and Chiari osteotomies. .
2.4
Arthroscopy
Arthroscopy is indicated for femoroacetabular impingement (FAI). It occurs when anatomic variation of the hip causes impingement between the femoral head–neck junction and the acetabular rim during functional motion. This condition is mainly seen in young and active men. Open or arthroscopic osteochondroplasty of the femoral head–neck junction is the surgical treatment for symptomatic cam impingement. Depending on the surgeon, it may be performed with an anterior open approach with or without arthroscopy by surgical dislocation or by arthroscopy exclusively. Good to excellent results are reported in 70 to 95% of patients.
2.5
THR
THR has been coined the “operation of the century”. Millions of THRs are performed worldwide to treat OA, with more than 95% of patients entirely satisfied with the functional results . The modern hip replacement was developed by Sir John Charnley in the 1960s and still represents the gold standard . However, significant improvements have been made over the last 50 years. The operation is performed now through a 6- to 8-cm incision and the patient stays about 3 nights in hospital, and just a few days after the surgery, can expect to walk normally with no walking aids and have a painless joint. Patients should not require revision for the next decades, if ever, and are free to return to complete activity including sports. There are few technical considerations, which we briefly discuss.
2.6
Bearing surfaces
The hip joint replacement is a ball-and-socket joint: it has a femoral head; the ball articulates the socket by a cup in the acetabulum. The materials in contact with each other are called bearing surfaces. Bearing surfaces are prone to wear, which may generate particulate debris and cause bone resorption and implant failure over time. Metal on polyethylene remains the most favored material among surgeons. It is cheap and easily machined in sizes and shapes. The latest developments such as highly crosslinked polyethylene have greatly decreased wear rates and almost obliterated the risk of particulate-induced osteolysis . Other bearings exist. Ceramic-on-ceramic bearings have been developed to avoid the wear problems with polyethylene. Indeed, there is no clinically measurable wear with this bearing. Nevertheless, this material has a risk of fracture < 1% . Metal-on-metal bearings are seldom used today because of the additional risks of adverse reaction to metal debris and metal ion in blood circulation and renal excretion.
2.7
Cemented and uncemented fixation
Two fixation methods exist, cemented and uncemented. Both are applicable to femoral stem and acetabular component. The results are similar and the preference for one or the other is mainly due to the surgeon or centre. In older patients, cemented fixation should be preferred because of the risk of fracture or non-integration of uncemented implants .
2.8
THR indications
THR is indicated with end-stage hip arthritis, when medical treatment has become ineffective, after an observation period of several weeks to several months. The excellent results of this procedure have widened its indications. Initially used exclusively with arthritis, it is today used in multiple situations such as osteonecrosis, secondary degenerative joint disease, congenital dislocation, hip fusion, bone tumor, hereditary disorders, and fractures of the femoral neck.
2.9
THR techniques
The surgery can be performed with various approaches. Each approach has relative advantages and drawbacks. The choice depends on the surgeon’s experience and choice and sometimes the anatomical characteristics of the patient. Recently, mini-invasive surgery (MIS) has permitted rapid recovery after the procedure. MIS decreases soft-tissue trauma, while allowing for adequate positioning of the prosthetic components. It contributes to dynamic stabilization of the hip . Some patients present complex hip cases such as developmental dysplasia of the hip, post-traumatic arthritis, or Legg-Calve-Perthes disease sequelae. In these cases, surgical techniques are more elaborate, and custom-made femoral implants may be necessary ( Fig. 2 ).

Related posts:
 Cartilage tissue engineering: From biomaterials and stem cells to osteoarthritis treatments
Osteoarthritis, obesity and type 2 diabetes: The weight of waist circumference
Osteoarthritis biomarkers derived from cartilage extracellular matrix: Current status and future perspectives
Osteoarthritis guidelines: Barriers to implementation and solutions
Spa therapy and knee osteoarthritis: A systematic review
Isokinetic muscle strengthening for knee osteoarthritis: A systematic review of randomized controlled trials with meta-analysis
Cartilage tissue engineering: From biomaterials and stem cells to osteoarthritis treatments
Osteoarthritis, obesity and type 2 diabetes: The weight of waist circumference
Osteoarthritis biomarkers derived from cartilage extracellular matrix: Current status and future perspectives
Osteoarthritis guidelines: Barriers to implementation and solutions
Spa therapy and knee osteoarthritis: A systematic review
Isokinetic muscle strengthening for knee osteoarthritis: A systematic review of randomized controlled trials with meta-analysis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


