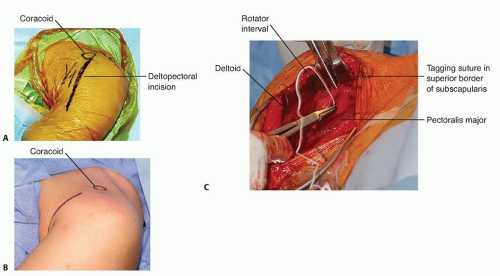
Incision begins inferior to the tip of the coracoid and progresses toward the anterior axillary fold.
FIG 1 • A. Deltopectoral incision. B. Axillary incision beginning inferior to the tip of the coracoid and progressing toward the anterior axillary fold. C. In this dissection, the subscapularis tendon is being tagged at the superior border of the rotator interval.
Internervous Plane
Deltoid muscle is supplied by the axillary nerve.
Pectoralis major muscle is supplied by medial and lateral pectoral nerves.
Surgical Dissection
Skin flaps are developed around the deltopectoral interval.
The deltopectoral interval, with its cephalic vein, is identified.
The deltopectoral interval is developed by retracting the pectoralis major medially and the deltoid laterally.
Vein may be retracted either medially or laterally.
We prefer to take it laterally, as fewer tributaries are disrupted.
The lateral border of the conjoint tendon is identified and the short head of the biceps (supplied by the musculocutaneous nerve) and coracobrachialis (supplied by the musculocutaneous nerve) are retracted medially to allow access to the anterior aspect of the shoulder joint.
Simple medial retraction of the conjoined tendon may be enough for a procedure such as subscapularis repair or capsular repair.
If more exposure is necessary, the conjoint tendon can be detached with the tip of the coracoid process.
The axillary artery is surrounded by cords of brachial plexus, which lie behind the pectoralis minor muscle.
To minimize risk for nerve injury, the arm should be kept adducted while work is being done around the coracoid process.
Remember, the musculocutaneous nerve enters the coracobrachialis on its medial side.
Overly aggressive retraction can cause a neurapraxia of the musculocutaneous nerve.
Behind the conjoined tendon of the coracobrachialis and the short head of biceps lies the subscapularis muscle.
Externally rotating the arm brings the subscapularis further into the operative field.
This maneuver increases the distance between the subscapularis and axillary nerve as it disappears below the lower border of the muscle.
Identifiable landmarks on the inferior border of the subscapularis are three small vessels (from the anterior humeral circumflex artery) that run transversely and often require ligation or cauterization.
These vessels run as a triad (often called the three sisters): a small artery with its two surrounding venae comitantes.
The superior border of the subscapularis muscle blends in with the fibers of the supraspinatus muscle in the rotator interval (FIG 1C).
The tendon of the subscapularis is tagged with stay sutures.
There are various ways of taking down the subscapularis as per surgeon preference.
Some divide the subscapularis 1 to 2 cm from its insertion onto the lesser tuberosity.
Some detach this insertion with a small flake of bone using an osteotome.
Some release the insertion subperiosteally directly from its insertion onto the lesser tuberosity.
The inferior border of the subscapularis is the easiest location to allow separation between the subscapularis and capsule.
The capsule is incised longitudinally to enter the joint wherever the selected repair must be performed.
PEARLS AND PITFALLS
Axillary nerve
▪ The axillary nerve branches off the posterior cord of the brachial plexus and transverses under the subscapularis muscle posteriorly through the quadrilateral space. Traction or excessive inferomedial dissection can place the nerve at risk.
Musculocutaneous nerve
▪ The musculocutaneous nerve branches off the lateral cord and enters the medial aspect of the conjoint tendon about 5 cm distal to the coracoid. Excessive retraction on the conjoint tendon can lead to nerve palsy.
Axillary artery and brachial plexus
▪ The axillary artery and brachial plexus course medially to the coracoid. Dissection medial to the coracoid will place these structures at risk.
ANTEROSUPERIOR APPROACH TO THE SHOULDER
Indications
Rotator cuff repair
Subacromial decompression of the shoulder
Acromioclavicular reconstructions
Open reduction and internal fixation (ORIF) of greater tuberosity fractures
Removal of calcific deposits from the subacromial bursa
Reverse shoulder replacement
Intramedullary nailing of humerus fractures
Incision
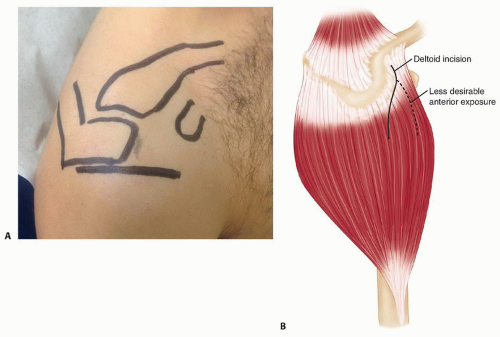
An incision is made paralleling the lateral acromion that begins at the anterolateral corner of the acromion and ends just lateral to the tip of the coracoid (FIG 2A).
Internervous Plane
The deltoid muscle is detached proximal to its nerve supply; therefore, there is no internervous plane with this approach.
Surgical Dissection
The incision is deepened to the deep deltoid fascia.
Subcutaneous flaps are raised.
The location of the deltoid split depends on the pathology being managed. When the pathology requires more exposure, moving the deltoid split posteriorly will improve exposure (FIG 2B).
Subperiosteally, the anterior deltoid is elevated from the acromion and the acromioclavicular joint. Continue the detachment by sharp dissection laterally to expose the anterior aspect of the acromion.
Bleeding will be encountered during this dissection as a result of the division of the acromial branch of the coracoacromial artery.
The surgeon should not detach more of the deltoid than is necessary.
The deltoid split is extended 2 to 3 cm distal to the acromion.
Stay sutures are inserted in the apex of the split to prevent the muscle from inadvertently splitting distally during retraction and damaging the axillary nerve.
The split edges of the deltoid muscle are retracted to reveal the underlying coracoacromial ligament.
The coracoacromial ligament is detached from the acromion by sharp dissection.
The supraspinatus tendon with its overlying subacromial bursa now can be visualized.
The head of the humerus is rotated to expose different portions of the rotator cuff.
FIG 2 • A. Anterosuperior approach to the shoulder. A transverse incision begins at the anterolateral corner of the acromion and ends just lateral to the coracoid. B. The posterior curve of the deltoid incision can be moved more posteriorly, as depicted here, to allow necessary exposure as dictated by the pathology.
PEARLS AND PITFALLS
Axillary nerve
▪ The axillary nerve runs beneath the deltoid muscle 4.3-8.2 cm distal to the angle of the acromion. A deltoid split distal to this point may injury the nerve.
Deltoid dehiscence
▪ Deltoid dehiscence may occur following this approach and the deltoid should be reattached using heavy, nonabsorbable sutures through bone tunnels in the acromion.
POSTERIOR APPROACH TO THE SHOULDER
Indications
Repair in cases of recurrent posterior dislocation or subluxation of the shoulder
Glenoid osteotomy
Treatment of fractures of the scapular neck
Treatment of posterior fracture and dislocations of the proximal humerus
Spinoglenoid notch cyst drainage
Incision
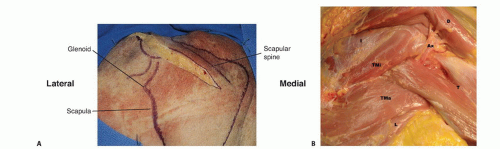
A horizontal incision is made along the scapular spine extending to the posterolateral corner of the acromion (FIG 3A).
For extensile exposure to the scapula, the incision can be continued distally along the medial border of the scapula (Judet approach).
Internervous Plane
Between teres minor (axillary nerve) and infraspinatus (suprascapular nerve)
The suprascapular nerve passes around the base of the spine of the scapula as it runs from the supraspinatus fossa to the infraspinatus fossa.
Surgical Dissection
The origin of the deltoid is identified on the scapular spine. There are three ways to manage the deltoid during posterior exposures:
Detach the origin on the scapular spine.
Split the deltoid muscle along the length of its fibers.
Elevate the deltoid from the inferior margin.
The plane between the deltoid muscle and the underlying infraspinatus muscle is identified.
The plane is easier to locate at the lateral end of the incision.
The internervous plane between the infraspinatus and teres minor muscles is identified (FIG 3B).
The axillary nerve runs longitudinally in the quadrangular space beneath the teres minor.
The posterior circumflex humeral artery runs with the axillary nerve in the quadrangular space between the inferior border of the teres minor muscle and the superior boarder of the teres major muscle.
The infraspinatus is retracted superiorly and the teres minor inferiorly to reach the posterior regions of the glenoid cavity and the neck of the scapula.
The posteroinferior corner of the shoulder joint capsule should be visible.
FIG 3 • A. Horizontal incision along the scapular spine allowing for the posterior approach to the shoulder. B. Cadaveric specimen depicting the internervous plane between the infraspinatus and teres minor as well as the axillary nerve in the quadrangular space. (A: From Goss TP. Glenoid fractures: open reduction and internal fixation. In: Wiss DA, ed. Master Techniques in Orthopaedic Surgery: Fractures, ed 2. Philadelphia: Lippincott Williams & Wilkins, 1998:3-17; B: Courtesy of Jesse A. McCarron, MD, Michael Codsi, MD, and Joseph P. Iannotti, MD.)
PEARLS AND PITFALLS
Suprascapular nerve
▪ Identifying the internervous plane between the infraspinatus and teres minor is critical and not always easy to visualize. Retraction of the infraspinatus muscle belly superiorly should protect the suprascapular nerve.
Axillary nerve and posterior circumflex humeral vessel
▪ Maintaining the surgical dissection superior to the teres minor and medial to the long head of the triceps should protect these structures.
HUMERUS APPROACHES
ANTERIOR APPROACH TO THE HUMERUS
Indications
Internal fixation of fractures of the humerus
Management of humeral nonunions
Osteotomy of the humerus
Incision
A longitudinal incision is made over the tip of the coracoid process of the scapula; it runs distally and laterally in the line of the deltopectoral interval to the insertion of the deltoid muscle on the lateral aspect of the humerus, about halfway down its shaft.
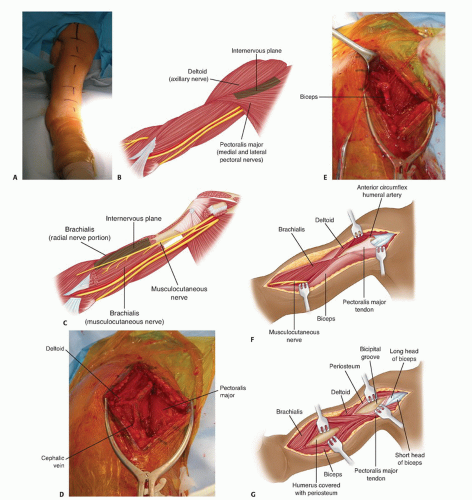
The incision should be continued distally as far as necessary, following the lateral border of the biceps muscle (FIG 4A).
Internervous Plane
The anterior approach uses two different internervous planes.
Proximally, the plane lies between the deltoid muscle (supplied by axillary nerve) and the pectoralis major muscle (supplied by medial and lateral pectoral nerves) (FIG 4B).
Distally, the plane lies between the medial fibers of the brachialis muscle (musculocutaneous nerve) and the lateral fibers of the brachialis muscle (radial nerve) (FIG 4C).
Surgical Dissection
Proximal Humeral Shaft
The deltopectoral interval is identified using the cephalic vein as a guide and the two muscles are separated, retracting the cephalic vein either medially with the pectoralis major or laterally with the deltoid.
The muscular interval is developed distally down to the insertion of the deltoid into the deltoid tuberosity and the insertion of the pectoralis major into the lateral lip of the bicipital groove (FIG 4D,E).
To expose the bone fully, the surgeon may need to detach part or all of the insertion of pectoralis major muscle.
The minimum amount of soft tissue should be detached to allow adequate visualization and reduction of the fracture.
If further exposure is needed, the surgeon dissects medially in a subperiosteal manner to avoid damage to the radial nerve, which lies in the spiral groove of the humerus and crosses the back of the middle third of the bone in a medial to lateral direction.
Distal Humeral Shaft
The surgeon identifies the muscular interval between the biceps brachii and brachialis.
The interval is developed by retracting the biceps medially (FIG 4F).
Beneath it lies the brachialis muscle, which covers the humeral shaft.
The fibers of the brachialis are split longitudinally in the interval between the medial two-thirds and the lateral one-third to expose the periosteum on the anterior surface of the humeral shaft.
The periosteum is incised longitudinally in line with the muscle dissection, and the brachialis is stripped off the anterior surface of the bone (FIG 4G).
In the anterior compartment of the distal third of the arm, the radial nerve pierces the lateral intermuscular septum and lies between the brachioradialis and brachialis muscles.
FIG 4 • A. Patient prepared for an anterior approach to the humerus. B. The internervous plane between the deltoid muscle and the pectoralis major muscle. C. Further distally, one can appreciate the internervous plane between the medial fibers of the brachialis (musculocutaneous nerve) medially and the lateral fibers of the brachialis (radial nerve) laterally. D. Deltopectoral incision: developing the interval between the deltoid and pectoralis major. The cephalic vein can be seen separating these two structures. E. With deeper dissection, the biceps tendon is seen running in the rotator interval. F. Further distal dissection reveals the musculocutaneous nerve passing along the medial border of the biceps muscle. G. To expose the distal third of the humerus, the fibers of the brachialis are split. Flexion of the elbow will relieve the tension off the brachialis, making the exposure easier. (A: Courtesy of Matthew J. Garberina, MD, and Charles L. Getz, MD.)
PEARLS AND PITFALLS
Musculocutaneous nerve
▪ Proximally, the risks are the same as the deltopectoral approach.
▪ Distally, the nerve can be found running between the biceps brachii and the brachialis. Locally, the nerve innervates the biceps brachii and the medial aspect of the brachialis. During this exposure, the biceps brachii should be retracted medially and the brachialis split in the midline of the muscle belly. The brachialis is dually innervated by the musculocutaneous nerve medially and the radial nerve laterally.
Radial nerve
▪ Proximally, the risks are the same as the deltopectoral approach.
▪ Distally, the nerve runs posterior to the humerus in the spiral groove and innervates the lateral aspect of the brachialis. Splitting the brachialis in the midline protects the nerve. In cases of open reduction, the nerve must be visualized prior to reduction, as it can become incarcerated between fracture fragments.
POSTERIOR APPROACH TO THE HUMERUS
Indications
ORIF of a fracture of the humerus
Treatment of nonunion
Exploration of the radial nerve in the spiral groove
Incision
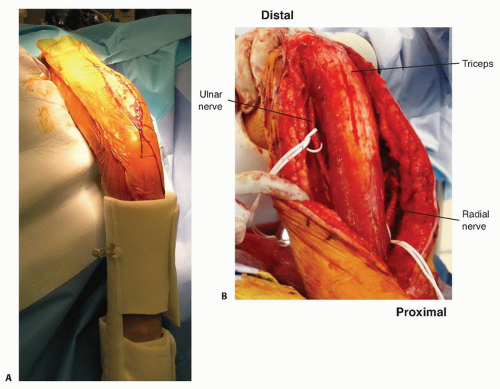
A longitudinal incision is made in the midline of the posterior aspect of the arm, from 8 cm below the acromion to the olecranon fossa (FIG 5A).
Internervous Plane
There is no true internervous plane; dissection involves separating the heads of the triceps brachii muscles, all of which are supplied by the radial nerve.
The medial head, which is the deepest, has a dual nerve supply (radial and ulnar nerves).
FIG 5 • A. Posterior approach to the humerus, showing the longitudinal incision along the midline of the posterior aspect of the arm. B. Once the outer layer of the triceps is isolated, one can see the two heads, the lateral head and long head. (continued)
Surgical Dissection
The surgeon incises the deep fascia of the arm in line with the skin incision.
The triceps muscle has two layers.
The outer layer consists of two heads: The lateral head arises from the lateral lip of the spiral groove and the long head arises from the infraglenoid tubercle of the scapula (FIG 5B).
The inner layer consists of the medial head, which arises from the whole width of the posterior aspect of the humerus below the spiral groove all the way down to the distal fourth of the bone.
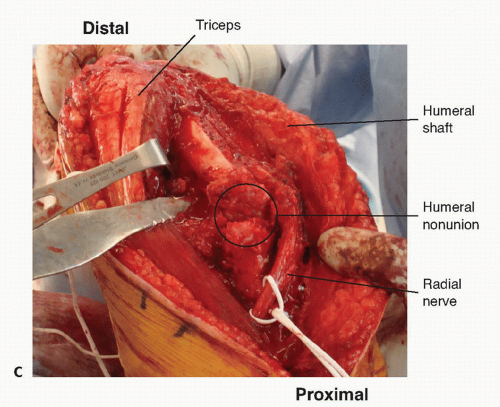
The spiral groove contains the radial nerve; the radial nerve separates the origins of the lateral and medial heads (FIG 5C).
To avoid iatrogenic nerve injury, the surgeon should never continue dissection down to bone in the proximal two-thirds of the arm until the radial nerve has been identified.
FIG 5 • (continued)C. In this humeral shaft nonunion, the triceps is reflected medially and the radial nerve can be seen passing through the spiral groove. (A: Courtesy of Matthew J. Garberina, MD, and Charles L. Getz, MD.)
MODIFIED POSTERIOR APPROACH TO THE HUMERUS
Indications
ORIF of humeral shaft fractures
ORIF of lateral condyle fractures
Only gold members can continue reading. Log In or Register to continue
 Shoulder Arthroscopy: The Basics
Shoulder Arthroscopy: The Basics
 Treatment of Recurrent Posterior Shoulder Instability
Treatment of Recurrent Posterior Shoulder Instability
 Repair and Reconstruction of Acromioclavicular Injuries
Repair and Reconstruction of Acromioclavicular Injuries
 Snapping Scapula Syndrome
Snapping Scapula Syndrome
 Lateral Epicondylitis (Tennis Elbow) Arthroscopic Treatment
Lateral Epicondylitis (Tennis Elbow) Arthroscopic Treatment
 Open Reduction and Internal Fixation of Fracture-Dislocations of the Elbow with Complex Instability
Open Reduction and Internal Fixation of Fracture-Dislocations of the Elbow with Complex Instability




