Surgical Approaches to the Elbow
Luke S. Austin
Joseph A. Abboud
Matthew L. Ramsey
Gerald R. Williams Jr.
ELBOW APPROACHES
The surgical exposures described for the elbow are divided into posterior, medial, and lateral approaches. These descriptions denote the deep surgical interval employed (Table 1).
Often, these deep approaches can be performed through a direct medial or lateral skin incision. Alternately, a midline posterior incision can be used and then subcutaneous flaps can be created to access the deeper medial or lateral intervals.
POSTERIOR APPROACH TO THE ELBOW
Releasing the triceps attachment to the olecranon is not advisable, owing to the difficulty of adequate repair and possible disruption during rehabilitation. Today, there are four choices of posterior exposure:
Triceps splitting
Triceps reflecting
Triceps preserving
Olecranon osteotomy
Triceps-Splitting Approaches
Posterior Triceps-Splitting Approach (Campbell)
Care must be exercised to maintain the medial portion of the triceps expansion over the forearm fascia in continuity with the flexor carpi ulnaris.
Laterally, the anconeus and triceps are more stable, with less chance of disruption.
Indications
Total elbow arthroplasty
ORIF of distal humerus fracture
Removal of loose bodies
Table 1 Indications and Recommended and Alternative Surgical Approaches
Indication
Recommended Approach
Alternative Approach
Total elbow arthroplasty
Bryan-Morrey, extended Kocher
Gschwend et al, Campbell, and Wadsworth
Soft tissue reconstruction
Global
Kocher, Bryan-Morrey, and Hotchkiss
T intercondylar fracture
MacAusland with chevron olecranon osteotomy
Alonso-Llames
Radial head fracture
Kocher
Kaplan
Capitellum fracture
Kaplan extended lateral approach
Kocher with or without Kaplan
Coronoid fracture
Taylor and Scham
Hotchkiss
Extra-articular distal humerus fracture
Alonso-Llames
Bryan-Morrey, Campbell
Monteggia fracture-dislocation
Gordon
Boyd
Radioulnar synostosis excision
Kocher or Gordon
Boyd or Henry
Capsulectomies
Posterior exposure of the joint for ankylosis, sepsis, synovectomy, and ulnohumeral arthroplasty
Approach
Skin incision begins in the midline over the triceps, about 10 cm above the joint line, and is generally placed laterally or medially across the tip of the olecranon. It continues distally over the lateral aspect of the subcutaneous border of the proximal ulna for about 5 to 6 cm (FIG 1A).
Triceps is exposed, along with the proximal 4 cm of the ulna.
A midline incision is made through the triceps fascia and tendon as it is continued distally across the insertion of the triceps tendon at the tip of the olecranon and down the subcutaneous crest of the ulna (FIG 1B).
Triceps tendon and muscle are split longitudinally, exposing the distal humerus.
The anconeus is then reflected subperiosteally laterally, whereas the flexor carpi ulnaris is similarly retracted medially.
Insertion of the triceps is carefully released from the olecranon, leaving the extensor mechanism in continuity with the forearm fascia and muscles medially and laterally (FIG 1C).
Ulnar nerve is visualized and protected in the cubital tunnel.
Closure of the triceps fascia is required only proximal to the olecranon, but the insertion should be repaired to the olecranon with a suture passed through the ulna.
The incision is then closed in layers.
Triceps-Splitting, Tendon-Reflecting Approach (Van Gorder)
A variation of the technique described earlier
Allows lengthening of the triceps if necessary
Has been largely abandoned in favor of the triceps-reflecting techniques
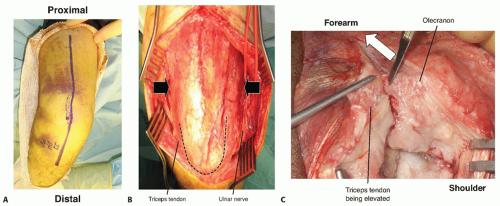 FIG 1 • A. Skin incision for the posterior triceps-splitting approach. B. Medial and lateral flaps are elevated, allowing full access to the triceps tendon. The ulnar nerve is isolated along the medial border with a vessel loop. C. The insertion of the triceps being elevated off the olecranon from medial to lateral. (A: Courtesy of Asif M. Ilyas, MD, and Jesse B. Jupiter, MD; B,C: Courtesy of Srinath Kamineni, MD.) |
Indications
Same as those for midline-splitting approach described earlier
Approach
A posterior midline incision begins 10 cm proximal to the olecranon and extends distally onto the subcutaneous border of the ulna between the anconeus and the flexor carpi ulnaris.
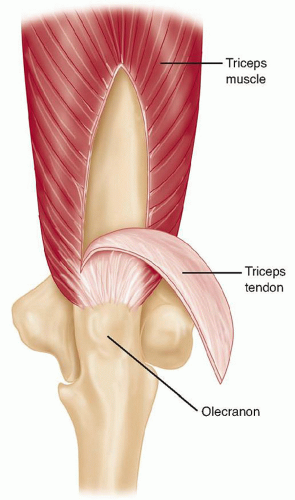
Triceps fascia and aponeurosis are exposed along the tendinous insertion into the ulna.
Tendon is reflected from the muscle in a proximal to distal direction, freeing the underlying muscle fibers while preserving the tendinous attachment to the olecranon (FIG 2).
Triceps muscle is then split in midline, and the distal humerus is exposed subperiosteally.
Periosteum and triceps are elevated for a distance of about 5 cm proximal to the olecranon fossa, exposing the posterior aspect of the joint.
If more extensive exposure is desired, the subperiosteal dissection is extended to the level of the joint, exposing the condyles both medially and laterally.
Ulnar nerve should be identified and protected.
After the procedure, if an elbow contracture has been corrected, the joint should be maximally flexed.
The tendon slides distally from its initial position, and the proximal muscle and tendon are reapproximated in the lengthened relationship.
The distal part of the triceps is then securely sutured to the fascia of the triceps expansion, and the remainder of the wound is closed in layers.
Triceps-Reflecting Approaches
The triceps mechanism may be preserved in continuity with the anconeus and simply reflected to one side or the other.
Three surgical approaches have been described that preserve the triceps muscle and tendon in continuity with the distal musculature of the forearm fascia and expose the entire joint.
Bryan-Morrey Posteromedial Triceps-Reflecting Approach
Developed to preserve the continuity of the triceps with the anconeus
Approach
A straight posterior incision is made medial to the midline, about 9 cm proximal and 8 cm distal to the tip of the olecranon (FIG 3A).
The ulnar nerve is identified proximally at the margin of the medial head of the triceps and, depending on the procedure, is either protected or carefully dissected to its first motor branch and transposed anteriorly.
The medial aspect of the triceps is elevated from the posterior capsule.
The fascia of the forearm between the anconeus and the flexor carpi ulnaris is incised distally for about 6 cm.
The triceps and the anconeus are elevated as one flap from medial to lateral, skeletonizing the olecranon and subcutaneous border of the ulna (FIG 3B). This should be performed at 20 to 30 degrees of flexion to relieve tension on the insertion, thereby facilitating dissection.
The collateral ligaments may be released from the humerus for exposure as needed (FIG 3C).
If stability is important, these ligaments should be preserved or anatomically repaired at the conclusion of the surgery.
When performing a linked total elbow replacement, it is not necessary to preserve or repair the collateral ligaments.
The triceps attachment can be thin at the attachment to the ulna, and it is not uncommon for a buttonhole to be created when reflecting the triceps.
To prevent this, the flap can be raised as an osteoperiosteal flap (see osteoanconeus flap approach).
A small osteotome is used to elevate the fascia with the petals of bone.
The flap is mobilized laterally, elevating the anconeus origin from the distal humerus until it can be folded over the lateral humeral condyle.
At this point, the radial head can be visualized.
The tip of the olecranon can be excised to help expose the trochlea.
Osteoanconeus Flap Approach
This provides excellent extension and reliable healing of the osseous attachment to the olecranon.
This approach exposes only the ulnar nerve, whereas the Mayo approach translocates the nerve.
Indications
This is a triceps-reflecting approach similar in concept to the Bryan-Morrey triceps-reflecting approach.
Most often used for joint replacement or distal humeral fractures
Approach
A straight posterior incision is made medial to the midline, about 9 cm proximal and 8 cm distal to the tip of the olecranon.
The ulnar nerve is identified and protected but not translocated.
The triceps attachment is released from the ulna by osteotomizing the attachment with a thin wafer of bone.
This is the essential difference from the Bryan-Morrey approach.
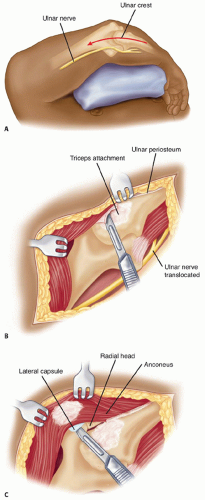
FIG 3 • The Bryan-Morrey posterior approach. A. Straight posterior skin incision. B. The ulnar nerve has been translocated anteriorly. The medial border of the triceps is identified and released, and the superficial forearm fascia is sharply incised to allow reflection of the fascia and periosteum from the proximal ulna. C. The extensor mechanism has been reflected laterally, and the collateral ligaments have been released.
The medial aspect of the triceps, in continuity with the anconeus, is elevated from the ulna (FIG 4A,B).
The collateral ligaments are either maintained or released, depending on the pathology being addressed and the need for stability.
After the surgical procedure, the wafer of bone is secured to its bed by nonabsorbable sutures placed through bone holes (FIG 4C).
Interrupted sutures are used to repair the remaining distal portion of the extensor mechanism.
Extensile Kocher Posterolateral Triceps-Reflecting Approach
Indications
Related posts:
 Open Reduction and Internal Fixation of Pediatric T-Condylar Fractures
Elbow Replacement for Acute Trauma
Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures
Fragment-Specific Fixation of Distal Radius Fractures
Vascularized Bone Grafting and Capitate Shortening Osteotomy for Treatment of Kienböck Disease
Operative Treatment of Metacarpal Fractures
Open Reduction and Internal Fixation of Pediatric T-Condylar Fractures
Elbow Replacement for Acute Trauma
Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures
Fragment-Specific Fixation of Distal Radius Fractures
Vascularized Bone Grafting and Capitate Shortening Osteotomy for Treatment of Kienböck Disease
Operative Treatment of Metacarpal Fractures
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


