Supracondylar Humeral Osteotomy for Correction of Cubitus Varus
Yi-Meng Yen
Richard E. Bowen
Norman Y. Otsuka
DEFINITION
Cubitus varus is a deformity of the distal humerus that results in a change in the carrying angle from physiologic valgus alignment between the upper arm and forearm.
Historically, before modern pinning techniques, cubitus varus was the most common complication following supracondylar humerus fracture, with an average reported frequency of 30%, with rates as high as 60%.
The appearance of the deformity is the major concern for the parents and patient, as there is little functional deficit.4
ANATOMY
Bone
The distal humerus consists of two structural columns of bone medially and laterally.
The olecranon and coronoid fossae separate the two structural columns.
The cortices of the distal humerus are thinner in the child than the adult, and the anteroposterior (AP) diameter of the distal humerus is decreased in children.
Neurovascular
The median nerve and brachial artery run along the medial border of the biceps brachii muscle in the upper arm and come to lie anterior and slightly medial in the cubital fossa.
The radial nerve enters the anterior compartment of the arm in the distal third of the upper arm and travels between the brachialis and brachioradialis over the anterolateral distal humerus before it enters the supinator muscle in the proximal forearm. There have been reports of the radial nerve enclosed within the callus of a supracondylar fracture.
PATHOGENESIS
Cubitus varus occurs predominantly because of a malunited supracondylar humerus fracture. Unequal growth of the distal humerus can cause cubitus varus, particularly medial physeal growth arrest.
The primary cause is coronal varus angulation of the distal humeral metaphysis.
Varus angulation can be caused by medial column comminution, causing the fracture to collapse into varus. Varus angulation can rarely be caused by lateral gaping at the fracture site.
Other coexisting deformities can exist with cubitus varus, including extension and internal rotation of the distal fragment.7
NATURAL HISTORY
The deformity is usually static and does not evolve with time, unless caused by a medial physeal disturbance.
The deformity is often not appreciated until several months after the fracture heals and the elbow flexion contracture that results from casting resolves.
Tardy ulnar nerve palsy may occur, owing to compression by chronic malpositioning of the triceps muscle due to a shift of the olecranon in the olecranon fossa.
Significant cubitus varus may contribute to elbow discomfort and posterolateral rotatory instability.
There may be a slight increased risk of subsequent lateral condyle fractures in children with cubitus varus.1
PATIENT HISTORY AND PHYSICAL FINDINGS
A detailed history is essential to understand parental and patient expectations of treatment in cubitus varus.
Physical findings include a varus change in the carrying angle when compared to the opposite, unaffected side.
Elbow and forearm range of motion should be documented.
A thorough examination of nerve function to the forearm and hand should be performed.
Hyperextension of the elbow indicates coexisting extension deformity at the malunion site.
A loss of external rotation can be due to shoulder pathology or due to an internal rotation malunion at the distal humerus.
The difference in carrying angle between the affected and unaffected side is the amount of cubitus varus.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Plain AP and lateral radiographs of the affected elbow should be obtained (FIG 1).
Additionally, an AP radiograph of the affected and unaffected elbow in full extension and supination that includes the distal humerus, forearm, and wrist should be obtained. This is used to plan the amount of surgical correction desired.
Advanced imaging (magnetic resonance imaging [MRI] of the elbow) may be of value in young children where distal humeral growth disturbance is suspected.3
DIFFERENTIAL DIAGNOSIS
Medial humeral condylar or trochlear growth disturbance
Malunited lateral humeral condyle fracture
Congenital dislocation of the radial head
Malunited fracture/separation of the distal humeral physis
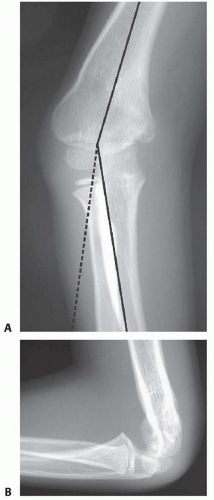 FIG 1 • A,B. AP and lateral radiographs obtained preoperatively for a patient with cubitus varus. |
NONOPERATIVE MANAGEMENT
Nonoperative management does not affect the appearance of cubitus varus.
If correction is contemplated, surgery should be undertaken at least 1 year after injury to ensure that there is no evidence of distal humeral avascular necrosis.
SURGICAL MANAGEMENT
Indications
Skeletally immature child with posttraumatic cubitus varus
Full elbow extension and flexion to at least 130 degrees
Child and family unaccepting of the appearance of the elbow
At least 1 year after initial injury
Goals
Correction of the carrying angle to equal the contralateral side7
In our experience, rotational deformity less than 45 degrees is well compensated for by shoulder and forearm rotation and does not need to be addressed in the osteotomy.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








