Submuscular Plating of Pediatric Femur Fractures
Ernest L. Sink
Benjamin F. Ricciardi
DEFINITION
Submuscular bridge plating is a minimally invasive, soft tissue preserving approach that provides relative stability for length-unstable pediatric diaphyseal femur fractures.
ANATOMY
The distal margin of the vastus lateralis is deep to the iliotibial fascia in line with the proximal pole of the patella.
The fibers of the distal vastus lateralis are oblique, and the muscle is not attached to the bone, providing a plane between the muscle and lateral periosteum of the femur for plate insertion.
PATHOGENESIS
NATURAL HISTORY/BACKGROUND
Femur fractures are the most common cause of hospital admission due to orthopaedic trauma for pediatric patients.6
Male patients are more commonly affected relative to female patients, and there is a bimodal age distribution with peaks in young (younger than 4 years old) patients and adolescent patients.
Fracture of the femoral diaphysis is more common than trochanteric or distal femoral locations.
PATIENT HISTORY AND PHYSICAL FINDINGS
History should include age, mechanism of injury (rule out child abuse in patients younger than 2 years old), other locations of pain to rule out concomitant injury, and relevant medical or family history (eg, cerebral palsy and osteogenesis imperfecta increase the risk of low-energy femur fractures).
Physical examination reveals shortening and rotational deformity of the affected extremity with painful range of motion. Neurovascular examination, skin integrity, signs of compartment syndrome should all be carefully assessed.
Concomitant injury should be ruled out because pediatric femur fractures represent high-energy injuries in many cases and can be associated with neurologic, visceral, and other musculoskeletal trauma.
IMAGING AND OTHER DIAGNOSTIC STUDIES
An anteroposterior (AP) and lateral view of the injured femur will diagnose the fractured femur. Imaging should include radiographs of the ipsilateral hip and knee to rule out secondary injuries to the femoral neck or knee joint.
SURGICAL MANAGEMENT
Operative stabilization is the treatment of choice for pediatric femur fractures in most children 5 years and older through skeletal maturity. Flexible elastic nailing is successful for the majority of diaphyseal femur fractures.1, 3 Factors such as comminution, long oblique length-unstable fractures, and children older than the age of 10 years have resulted in increased complication rates in some series with flexible elastic nailing.7, 10 Therefore, alternative means of stabilization have been suggested for fractures with these characteristics.
Plate osteosynthesis is a proven method to stabilize pediatric fractures. The use of submuscular bridge plating for comminuted femur fractures allows for rigid stabilization, minimally invasive techniques, avoidance of avascular necrosis (AVN) of the femoral head, and stabilization of the diaphyseal/metaphyseal junction.
The procedure is indicated for patients 5 years old to skeletal maturity. The fracture patterns most amenable to bridge plating are comminuted or long oblique length-unstable fractures. Older or heavier children with femoral canals unable to accommodate an intramedullary (IM) nail would also be appropriate candidates (FIG 1).
Submuscular plating is also a reliable option for proximal or distal one-third femur fractures.1 For these fractures, there needs to be room for two to three screws in the proximal or distal diaphyseal region.
It has a relative contraindication in patients that have transverse fractures. We prefer flexible IM nails to bridge plating for transverse or short oblique mid-diaphyseal fractures.
Preoperative Planning
All patients should be carefully evaluated for other injuries including knee or hip injuries.
An operating room equipped with traction bed and fluoroscopy is critical.
No preoperative templating is required, as the plate length and contour are chosen under sterile conditions.
It is important to have the long plates available and the appropriate screw set.
Finally, evaluating the natural rotation of the contralateral leg is useful as a reference prior to draping.
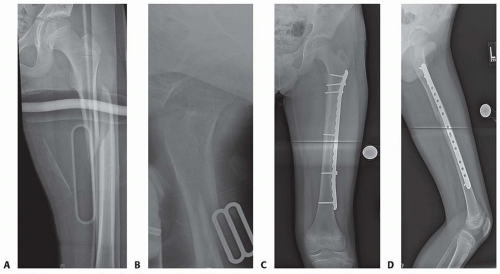
FIG 1 • A,B. Displaced pediatric diaphyseal femur fracture in AP and lateral planes, respectively. C,D. Submuscular bridge plating shows appropriate fracture reduction and restoration of length in in AP and lateral planes, respectively.
A narrow 4.5-mm plate is most often used.
This plate is readily available, easy to contour, and percutaneous screw placement is forgiving.
Many of the currently available implants have the locking or nonlocking screw option.
Although nonlocking screws have been successful, locking screws may have some benefit in osteopenic patients or very proximal or distal fractures, where there is little available room for screws.
In our experience, nonlocking screws achieve enough stability in this age group and allow easier percutaneous screw placement compared with locking screws.
If a locking plate is used, a combination of locking and nonlocking screws are needed to reduce the femur to the plate.
It may be easier to place the locking screws with direct plate exposure rather than percutaneous exposure.
Self-tapping screws are essential for easier percutaneous insertion.
In smaller children, a long, narrow 3.5-mm plate may be used if absolutely necessary, but a 4.5-mm plate will fit most femurs even in the younger children.
The plate length chosen is usually 10 to 16 holes, depending on fracture location and patient size.
The plate commonly spans from just below the greater trochanteric apophysis to the metaphysis of the distal femur.
If possible, the plate length should allow six screw holes proximal and distal to the fracture.
Positioning
Patients are positioned supine on a fracture table.
The normal contralateral leg is extended and slightly abducted to allow a true lateral fluoroscopic image of the fractured femur.
Alternatively, a “well-leg” holder may also be used.
Provisional reduction restoring femoral length and rotation is obtained with boot traction and verified fluoroscopically.
Final alignment is performed with plate fixation as described later.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








