Stepwise Approach to Equinus Deformity Correction with Circular External Fixation
Mikhail L. Samchukov
Alexander M. Cherkashin
Edgardo Rodriguez
John G. Birch
Introduction
Equinus deformity is generally defined as a limitation of dorsiflexion motion at the ankle joint resulting in inability of the heel to contact the ground surface without some form of anatomical or functional compensation in the lower limb and foot. Despite numerous publications on ankle equinus, there is no consensus regarding the degree of ankle dorsiflexion restriction required to constitute a diagnosis of “equinus deformity,” nor a standardized method of the measurement of ankle equinus. The reported range of normal ankle joint dorsiflexion varies from 3 to 15 degrees in full knee extension and from 10 to 20 degrees or even greater at 90 degrees of knee flexion.1–7 As a result, a wide range of reduced ankle dorsiflexion has been considered as constituting equinus deformity, varying from less than 0 degree to less than 10 degrees of dorsiflexion.8–12
Some authors have suggested using the tibial–sole angle (TSA), calculated as an angle between the line drawn from the plantar aspect of the first metatarsal to the plantar aspect of the calcaneus and the line drawn along the longitudinal axis of the tibia on a weight bearing lateral radiograph.13 Equinus deformity is defined based on foot orientation in the sagittal plane relative to its normal neutral position (TSA = 90 degrees). Equinus deformity is considered to be mild when the foot is in a position of plantarflexion less than 20 degrees from neutral, moderate when from 20 to 40 degrees, and severe when more than 40 degrees.14 Other authors recommend using the tibiotalar angle (TTA), the angle between the tibial anatomical axis and the axis of the talus for deformity assessment. Foot orientation with TTA more than 115 degrees is considered to be true ankle equinus.15
Although the etiology of ankle equinus is still often poorly understood, a variety of potential causes can be identified including (1) congenital anomalies such as cerebral palsy, Charcot–Marie–Tooth disease, myelomeningocele, arthrogryposis, clubfoot, muscular dystrophy, flatfoot, fibular hemimelia, limb length discrepancy, and idiopathic toe walking, and (2) acquired or compensatory deformities from poliomyelitis, trauma, burns, limb lengthening, and contracture resulting from immobilization after trauma. Multiple factors may contribute to ankle equinus including soft tissue (ankle equinus contracture), adjacent joints, and associated foot and tibial osseous deformities.
Typically, conservative treatment is initially used to manage equinus. Depending on the etiology of the equinus, different conservative modalities including physical therapy, kinesiotaping, orthoses, chemodenervation (intramuscular injections of botulinum toxin type A, alcohol, or phenol), nerve neurotomy, and serial casting may be indicated.16,17 If conservative treatment is no longer effective, the patient can undergo surgical correction including ankle and/or subtalar joint release, tendon lengthening, fascial lengthening, or tendon transfers followed by acute deformity correction.
In patients with equinus contracture, tendon Achilles lengthening (TAL) can be performed via either open Z-lengthening or percutaneous incomplete tenotomies. In open techniques, a posterior longitudinal incision is performed, the tendon is cut in a Z-shaped fashion, the foot is dorsiflexed resulting in longitudinal shifting of two portions of the tendon that are sutured together in the lengthened position followed by wound closure. With percutaneous techniques such as described by Hoke, two or three incomplete horizontal tenotomies are usually performed with a subsequent acute tendon stretching resulting in its lengthening within the tendon sheath. An alternative to TAL techniques is selective gastrocnemius fascia lengthening using surgical open or endoscopic muscle recession. In this case, the overlying fascia of the gastrocnemius is released allowing anatomical preservation of underlying muscle fibers of the gastrocnemius and soleus muscles. Several surgical procedures have been described for gastrocnemius recession and gastrocnemius–soleus recession to resolve equinus deformity including Baumann, Baker, Strayer, Vulpius, and Stoffel techniques.18–20
Despite the benefits of soft tissue lengthening techniques, such as the ease and rapidity of the surgical procedure and the
predictable improvement in ankle dorsiflexion, recurrence of equinus deformity may occur due to weakness of plantarflexion or calcaneal (crouch) gait may develop due to over lengthening.21–23 In addition, the open surgical techniques may lead to (1) significant prominent scar tissue formation provoking Achilles tendonosis, (2) sural neuropraxia due to posterior muscle stretch, and (3) inadvertent complete tenotomy. To prevent those complications, correction of more than 30 degrees should be avoided.18,20,24
predictable improvement in ankle dorsiflexion, recurrence of equinus deformity may occur due to weakness of plantarflexion or calcaneal (crouch) gait may develop due to over lengthening.21–23 In addition, the open surgical techniques may lead to (1) significant prominent scar tissue formation provoking Achilles tendonosis, (2) sural neuropraxia due to posterior muscle stretch, and (3) inadvertent complete tenotomy. To prevent those complications, correction of more than 30 degrees should be avoided.18,20,24
Gradual correction of the foot equinus position using circular or semicircular external fixation in combination with Ilizarov distraction histogenesis is an alternative method to acute deformity correction following open or percutaneous tendon lengthening and muscle recession. In this method, the soft tissues are slowly but progressively stretched rather than surgically released and stretched acutely, thereby avoiding traction nerve injuries and extensive scarring while more adequately adapting to new dimensions following controlled incremental movement of the osseous segments. In addition, external fixation offers more superior stabilization of the tibia and foot providing the possibility to combine equinus deformity correction with gradual distraction across the ankle joint and allowing the patient to ambulate during the treatment.
Indications
According to Ilizarov, foot deformity correction using circular external fixation can be divided into closed and open techniques.13,25 Closed techniques involve gradual stretching of soft tissues of the foot without osteotomies and are usually applied for correction of equinus contracture with relatively congruent articulating joint surfaces. This involves application of an external circular fixator that allows controlled gradual incremental dorsiflexion movement of the foot either through the natural or through the predetermined axis of rotation located in the talus.
Principal indications for closed gradual equinus deformity correction using circular external fixation include:
Severe equinus deformity with TTA more than 115 degrees without osseous deformities
Less severe equinus deformity with very stiff surrounding soft tissues when gradual correction is indicated to avoid neurovascular injury during acute deformity correction
Recurrent equinus deformity after failure of previous soft tissue releases and open surgical procedures
Open techniques are applicable in cases with compromised articulating surfaces and/or substantial bone deformities. In such cases, deformity correction is performed via various types of osteotomies followed by acute or gradual deformity correction. In addition, circular external fixation is used in cases with significantly compromised soft tissues when acute equinus deformity correction is indicated. In these cases, external fixation may be indicated to avoid infection after an open procedure with internal fixation and improve the stability of fixation with simultaneous reduction of compression forces on the joints.
Two major types of circular external fixators have been used for equinus correction including (1) Ilizarov-type modular external apparatus with associated Ilizarov method of gradual distraction and (2) octahedral variable-strut-length hexapod-type external fixator. This second type of external fixator requires the acquisition of numerous anatomic and frame-related parameters and intensive preoperative planning using associated software to program gradual foot movement during correction.
One well-known hexapod-type external fixator is the Taylor Spatial Frame or TSF (Smith & Nephew, Memphis, TN). Several TSF configurations have been described for foot deformity correction including standard ring constructs, miter and butt external fixation constructs.3,26–30 Several Ilizarov-type circular fixators have been described for management of ankle equinus. Since deformity is usually corrected via gradual movement through the predetermined axis of rotation, these external fixators include two special biomechanical modules-hinges with the static axis of rotation and angular distractor for gradual incremental distraction or compression. Those modules can be assembled from multiple individual components such as posts in the original Ilizarov external fixator (Smith & Nephew, Memphis, TN) and RingFix (SBi, Morrisville, PA) or provided as preassembled or universal components such as preassembled inline/outboard hinges and angular distractors in the Distraction Osteogenesis Ring System (Synthes, West Chester, PA) and TrueLok Ring Fixation System (Orthofix, Lewisville, TX). The circular external fixator used in all clinical examples of this chapter is the TrueLok Circular External Fixation System (Orthofix, Lewisville, TX). Irrespective of which external fixator is used, the principles of gradual equinus deformity correction remain the same for all circular external fixators.
Preoperative Considerations
Preoperative evaluation of ankle equinus deformity considered for Ilizarov-type of external fixator application includes detailed analysis of the deformity and identification of the location of the hinge axis relative to the natural axis of rotation of the ankle. For those purposes, the lateral radiograph of the affected foot and ankle is taken in the standing (weight-bearing) position. Several lines are drawn to analyze associated angles and determine components of the foot involved in ankle equinus deformity (Figure 22.1). These lines include (1) the anatomical axis of the tibia, (2) the distal tibia–ankle joint reference line, (3) the line representing the sole of the foot, connecting the plantar aspect of the head of the first metatarsal with the plantar aspect of the calcaneus, (4) the axis of the talus, (5) the axis of the calcaneus, and (6) the axis of the first metatarsal.
This is followed by measurement of the angles formed by the drawn lines and their interpretation. Those angles include (1) TSA between the tibial anatomical axis and the line representing the sole of the foot, (2) anterior distal tibial angle (ADTA) between the tibial anatomical axis and the distal tibial ankle joint reference line, (3) TTA between the tibial anatomical axis and the axis of the talus, (4) sole–talar angle (STA) between the axis of the talus and the line representing the foot sole, (5) talar–first metatarsal angle (Meary angle) between the axis of the talus and the axis of the first metatarsal, and (6) calcaneal–first metatarsal angle (cavus angle) between the axis of calcaneus and the axis of the talus.13,15
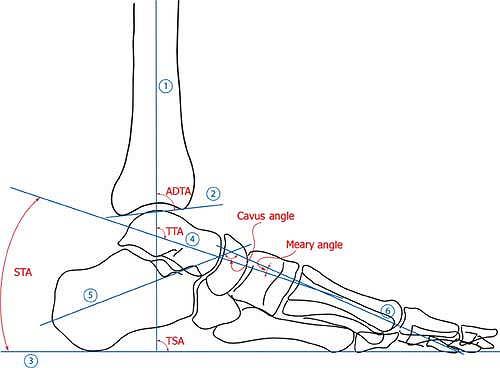 Figure 22.1. Outline of the distal tibia and foot from a lateral radiograph for preoperative evaluation of ankle equinus demonstrating anatomical axis of the tibia (1), distal tibial ankle joint reference line (2), foot sole line (3), axis of the talus (4), axis of calcaneus (5), and axis of the first metatarsal (6). ADTA, anterior distal tibial angle; Cavus angle, calcaneal–first metatarsal angle; Meary angle, talar–first metatarsal angle; STA, sole–talar angle; TSA, tibial–sole angle; TTA, tibiotalar angle. |
Angle analysis starts from the TSA. If the TSA is increased (normal TSA at neutral foot orientation is 90 degrees), the foot position can be interpreted as an equinus. Analysis of the other angles helps to identify whether the anatomical bony abnormality or functional imbalance are responsible for that equinus position and to localize this abnormality/imbalance. Result of this analysis will also influence decision making to determine appropriate treatment tactics to correct foot equinus.
For example, if the ADTA is increased (normal ADTA is 80 degrees, apex posteriorly), the equinus results from tibial sagittal plane deformity (procurvatum) and should be corrected via supramalleolar osteotomy. In cases with increased TTA (normal TTA is 115 degrees), the equinus is located at the level of the ankle joint and can be interpreted as a true ankle equinus. If the increase in TTA is proportional to the increase in TSA, the ankle equinus is solely responsible for foot equinus position. In patients with relatively congruent articulating joint surfaces, correction of equinus can be achieved using closed Ilizarov technique with hinges and angular distractor. In situations with compromised articulating surfaces, correction of equinus can be achieved using subtalar focal dome osteotomy followed by acute/gradual rotation of the foot into dorsiflexion.
In cases where increase in the TTA is not proportional to a TSA increase (usually TSA > TTA), other foot deformities are present and combined with ankle equinus. Ankle equinus may be combined with a calcaneal deformity manifested by decreased height of the calcaneus and reflected as decrease in the STA (normal STA is 24.5 degrees). Ankle equinus may also be combined with an anterior cavus deformity reflected as a decreased Meary angle (normal talar–first metatarsal angle is 5 degrees). Finally, when the TSA is increased but the TTA and STA are normal, the equinus foot position may result from cavus deformity represented by a decreased cavus angle (normal calcaneal–first metatarsal angle is 130 degrees). Depending on the severity of equinus in such cases, deformity correction can be achieved by one of the Ilizarov closed techniques or through the different forms of V-osteotomy and Y-osteotomy.
Detailed Surgical Techniques
Surgical technique and external fixator assembly mainly depend on the method of equinus deformity correction selected: (1) Closed method of gradual deformity correction either through the predetermined axis of rotation (two hinges with angular distractor) or through the natural axis of foot plantar/dorsiflexion at the talus (floating talus technique), or (2) open method of foot deformity correction using supramalleolar osteotomy, focal dome osteotomy, V-osteotomy, and Y-osteotomy followed by acute or gradual deformity correction.
Closed Method of Equinus Deformity Correction
The external fixator for closed gradual deformity correction can be assembled as either constrained or unconstrained hinge system.25,31,32 A constrained hinge system uses a static predetermined axis of rotation of the foot during equinus deformity correction, which is the common axis of rotation of both hinges on the external fixator. Foot rotation is achieved by acute manipulation or pre-calculated gradual incremental daily adjustments (distraction/compression) of the angular distractor.
An unconstrained hinge system uses the natural (anatomical) center of rotation of the ankle joint as the axis of foot rotation during the equinus deformity correction. Due to the multiaxial nature of the ankle joint and fluctuating orientation of the rotation center,33–38 the external fixator assembly has no hinges attached to the external fixator in relation to the center of rotation. In this case, foot rotation is usually achieved by gradual anterior compression, posterior distraction, or a combination of both.
Constrained Gradual Equinus Deformity Correction through the Predetermined Axis of Rotation using Hinges and an Angular Distractor
The external fixator for closed gradual deformity correction through the predetermined axis of rotation consists of two sections (tibial double-ring block and foot support) interconnected by two hinges (laterally and medially) and an angular distractor posteriorly. The tibial double-ring block is composed of two rings (usually of the same diameter) placed parallel to each other and connected by four threaded rods. The distal ring of the double-ring block is placed at the supramalleolar level while the proximal ring is located at the medial/proximal third of the limb. The minimal acceptable separation between the distal and proximal rings of the block should be approximately 100 mm. Initially (e.g., during the preoperative or intraoperative external fixation preassembly), two rings are connected to each other only anteriorly and posteriorly by two threaded rods that are utilized for external fixation alignment during the surgery. Medial and lateral threaded rods are attached at the end of the surgery to increase the external fixator’s rigidity and overall stability of fixation. In cases when equinus deformity correction is combined with tibial lengthening (Figure 22.2), an additional ring is attached to the external fixator proximally to the double-ring block. This ring is used to provide stable fixation of the proximal tibial segment after proximal tibial osteotomy for lengthening.
 Figure 22.2. Severe equinus deformity in a 15-year-old girl secondary to linear scleroderma associated with 4 cm of tibial shortening: (A) clinical photograph demonstrating foot equinus with no ankle motion, waxy texture of the skin on the tibia and dorsum of the foot with areas of hyperpigmentation; (B) lateral radiograph illustrating foot equinus with congruent articulating surfaces at the ankle joint; (C) intraoperative photograph showing foot stabilization with oblique wires; (D) intraoperative photograph demonstrating alignment of hinge axes by bending the distal tibial ring during external fixation assembly; (E) intraoperative radiograph illustrating hinge rotation axis aligned with the center of the talar dome; (F) clinical photograph of the final external fixation assembly showing its orientation relative to the tibial and foot axes; (G–I) postoperative radiographs and photograph demonstrating foot position before gradual equinus deformity correction; (J, K) postoperative radiographs demonstrating foot position after gradual equinus deformity correction; (L, M) anteroposterior and lateral radiographs after foot support removal during the consolidation period showing active mineralization of the 3 cm distraction regenerate; (N) clinical photograph after foot support removal illustrating plantigrade position of the foot; (O–Q) radiographs and clinical photograph at 2-year follow-up. |
Typical fixation of the double-ring block to the tibia for equinus deformity correction is achieved by two 1.8 mm diameter cross wires at the distal ring and one 5 mm diameter medial-face half-pin at the proximal ring. In order to protect the syndesmosis, one of the cross wires is an olive-stopper fibular-tibial wire inserted from posterolateral in an anteromedial direction, with the olive-stopper resting on the fibula. Depending on individual characteristics of the patient such as increased weight, large muscle mass, increased physical activity, involvement in athletics, and poor bone quality, stabilization of the tibial double-ring block can be supplemented by inserting a third wire at the distal ring and by either replacing the half-pin at the proximal ring with two wires, adding a second half-pin, or combining the first half-pin with a medial-face wire.
For foot support assembly, a foot plate with a double row of holes can be used in conjunction with a same diameter half ring connected to the foot plate anteriorly. Alternatively, a foot support can be constructed from a horseshoe-shaped foot plate with a single row of holes, two foot plate extensions to accommodate different lengths of the foot, and an anteriorly placed half ring.
Typical fixation of a foot support to bone is achieved by two 1.8 mm diameter calcaneal opposing olive-stopper wires (inserted inferior to the peroneal tendon laterally and inferior/posterior to the tarsal tunnel medially) and one 1.8 mm diameter medial olive-stopper wire inserted through the bases of at least the first and fifth metatarsals. Depending on the individual metatarsal relationships, a forefoot fixation wire can penetrate the first, second, and fifth; first, fourth, and fifth; or all five metatarsals. Forefoot stabilization can be increased by placing a second metatarsal lateral olive-stopper wire. In this case, the first forefoot wire is inserted through the first, second, and third metatarsals while the second wire penetrates the fifth and fourth metatarsals. The second forefoot wire is inserted at the base of the metatarsals and at a slightly oblique direction from inferior to superior and from posterior to anterior following the orientation of the metatarsals.13
Fixation of the hindfoot can also be increased by placing a third horizontal calcaneal wire and/or a midfoot wire through the cuboid and cuneiforms. Alternatively, two 5 mm diameter half-pins can be inserted posteriorly (the first half-pin from posterolateral to anteromedial, and the second half-pin from posteromedial to anterolateral) for calcaneal fixation of the hindfoot. Finally, two calcaneal-midfoot olive-stopper wires inserted in the calcaneus from the posterolateral and posteromedial toward anteromedially and anterolaterally, respectively, can be used for foot stabilization (Figure 22.2C). Those wires exit at the base of the metatarsals crossing the entire foot in the horizontal plane. In order to increase the stability of fixation further, they can be supplemented by two or three parallel wires placed horizontally through the calcaneus, midfoot, and/or metatarsals (Figure 22.2G). In some cases of rigid equinus deformity, digital wires can be inserted through the interphalangeal joints to prevent digital contractures during deformity correction.
Related posts:
 Biomechanics of External Fixation
Operating Room Preparation and External Fixation Equipment
Stepwise Approach to Midfoot/Hindfoot Trauma and External Fixation
Stepwise Approach to Uniplane, Biplane, Delta, and Hybrid External Fixation
Stepwise Approach to Charcot Hindfoot/Ankle Reconstruction and External Fixation
Stepwise Approach to Foot and Ankle Osteomyelitis and External Fixation
Biomechanics of External Fixation
Operating Room Preparation and External Fixation Equipment
Stepwise Approach to Midfoot/Hindfoot Trauma and External Fixation
Stepwise Approach to Uniplane, Biplane, Delta, and Hybrid External Fixation
Stepwise Approach to Charcot Hindfoot/Ankle Reconstruction and External Fixation
Stepwise Approach to Foot and Ankle Osteomyelitis and External Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


