Stepwise Approach to Bone Loss, Transport, and Lengthening with External Fixation
Vasilios D. Polyzois
Ioannis A. Ignatiadis
Alexandru V. Georgescu
Spyridon G. Pneumaticos
Introduction
Bone transport is perhaps one of the most unique innovations of the Ilizarov circular external fixation system. Smaller or larger bone and soft tissue defects resulting from traumatic or infectious processes can be treated with bone transport of a segment or segments of bone within the affected lower extremity. This technique is based on the distraction histogenesis phenomenon, which is characterized by nature’s capability to heal a fracture in diastasis and the ability to elongate skin, nerves, muscles, and vessels under gradual distraction. Bone transport is usually a salvage procedure in complex conditions where other procedures have failed and has proven effective when compared to conventional methods.
Bone transport was identified in the literature for decades as an alternative in the management of aseptic or septic and closed or open bone loss of the lower extremity. The terms segmental or internal lengthening are synonymous and indicate that although the proximal and distal anatomic structures are intact with normal length of the extremity, a loss of a fragment of bone (up to subtotal bone loss) possibly with its soft tissue envelope is in between or is necessary to be left behind after surgical debridement. Proximal and distal healthy anatomic structures may also involve different bones and the technique typically does not interfere with the length of the extremity.
Other alternative techniques to address severe bone and soft tissue loss of the lower extremity include and are not limited to vascularized fibular autografts, intramedullary nails with external fixation in combination with autografting and orthobiologics, structural allografts with autografts and orthobiologics, induced membrane techniques as well as free flaps, and autografting.
In this chapter, the authors will review different applications of the bone transport technique including isolated significant bone loss case scenarios or a combination of major bone and soft tissue loss in the lower extremity. Furthermore, the distraction histogenesis operative technique will be demonstrated solely or when performed in combination with other fixation methods or with traditional flap surgery and advanced plastic microsurgical techniques.
Preoperative Considerations
Careful preoperative planning is necessary to determine the bone segment that will be transported. One end of this segment is adjacent to the missing bone or to the bone that will be resected and it will engage the opposite end of the gap when the transport is complete. The other end is where the iatrogenic fracture (corticotomy) will take place to make the bone transport possible. The first mentioned end of the bone segment is the docking end and the other end is the trailing end of the transported segment of the bone. Behind the trailing end, by gradual distraction, the same dynamic process of new bone (regenerate bone) formation takes place, as in simple lengthening by intramembranous ossification. As the external fixator drives the docking end toward the opposite healthy fragment of bone, many obstacles may be present to block the way so that healing procedure starts between these two edges, that is, the docking site.
Some of the most common obstacles associated with the bone transport process include the formation of connective tissue within the segmental gap and soft tissue that can be interposed between the facing bone edges as well as the presence of poor pin placement of the external fixator without correct preoperative planning. In the event of no postoperative complications, the vascularization process of the facing bony edges will start normally and the shape of their surfaces plays a significant role for successful bone healing. In many cases, reshaping of the facing ends in a flat, cup or cone shape or even autografting may be necessary at the docking site. Additional orthobiologic materials may also be added at the docking site to enhance and promote further bone healing.
Ilizarov termed the above-described technique as bifocal for distraction at one level (corticotomy) and compression at a second level (the level of the pseudarthrosis). Depending on the
specific location of bone loss, the corticotomy can be proximal with distal transportation of the bone segment (Figure 21.1) or distal with proximal transportation of the bone segment (Figure 21.2).
specific location of bone loss, the corticotomy can be proximal with distal transportation of the bone segment (Figure 21.1) or distal with proximal transportation of the bone segment (Figure 21.2).
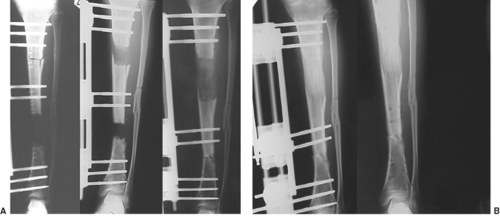 Figure 21.1. Proximal tibial corticotomy with distal transportation of a bone segment for the management of a severe tibial bone loss in the lower extremity (A). Note the use of a uniplane monolateral external fixator and final outcome (B). |
In addition, in certain case scenarios trifocal techniques (Figure 21.3) can be adapted and very rarely, quadrifocal techniques have been used in the literature. Quadrifocal bone transport is not routinely recommended due to an increased number of corticotomies that interfere with vascularization as well as the inevitably small bony segments that undergo transportation. In those severe cases of bone loss, a partial fibular transport with the posterior aspect of the fibula intact may be considered as an alternative to the bone transport technique. Although this procedure is very challenging, it may also provide a much faster regenerate bone than even a trifocal bone transport (Figure 21.4).
There are usually two different external fixation designs for the bone transport technique. The safest and most common types include the uniplane monolateral or multiplane circular external fixation systems. Uniplane monolateral external fixators are faster and easier to apply and their basic construct includes two clamps with Schanz pins attached on the healthy portions of the bone proximally and distally. In most cases, these are fixed on the rail and do not move during the bone transport procedure. In between the two clamps there is another clamp (rarely two when performing trifocal technique) with Schanz pins attached on the segment of bone that is being transported starting its way from the first fixed clamp toward the second fixed clamp. Careful planning and placement of the external fixation pins and/or wires is required in order to avoid hardware jamming and revisional surgery.
Inappropriate use of pin fixation may result in deviation of the transported segment and subsequent malformation of the bone transport technique. Unlike the circular external fixators, uniplane monolateral constructs are attached by only Schanz pins that transmit forces directly on the soft tissues for distraction and transportation together with the bone so distraction histogenesis is performed instead of a sole distraction osteogenesis. This feature of the large Schanz pins is also essential for the gradual closure of major open wounds and is also ideal for allowing possible concomitant plastic surgery procedures due to the increased space within the external fixation pins and clamps. Careful preoperative planning of pin insertion is necessary to avoid any unwanted deviation or inadequate bone segment transportation.
Circular external fixators are utilized for more complex bone transport procedures and are ideal for dynamic properties that differ from the static circular external fixators. Its indications are mostly considered for major bone and soft tissue loss. It usually takes only a small portion of bone segment for safe attachment of the most proximal and most distal fixed circular rings while uniplane monolateral external fixation needs the presence of at least the entire metaphyses for the attachment of the fixed clamps.
Surgical Technique
Significant Isolated Bone Loss with Adequate Soft Tissue Coverage
Although the soft tissue envelope is healthy in these case scenarios and only the bone segment loss needs to be addressed, extra caution is necessary during the bone transport and especially when the large diameter Schanz pins are utilized. In many cases, the soft tissues are extremely stretched and under tension and eventually end up in excessive soft tissue mass toward the docking site. This process is based on the dermogenesis created behind the trailing end of the
transported bone segment and needs to be addressed at each procedure. Regular skin releases under local anesthesia with the use of a no. 11 blade are usually necessary during the bone transport procedure. This technique can never be underestimated since excess skin tissue at the docking site can create major difficulties in bone healing.
transported bone segment and needs to be addressed at each procedure. Regular skin releases under local anesthesia with the use of a no. 11 blade are usually necessary during the bone transport procedure. This technique can never be underestimated since excess skin tissue at the docking site can create major difficulties in bone healing.
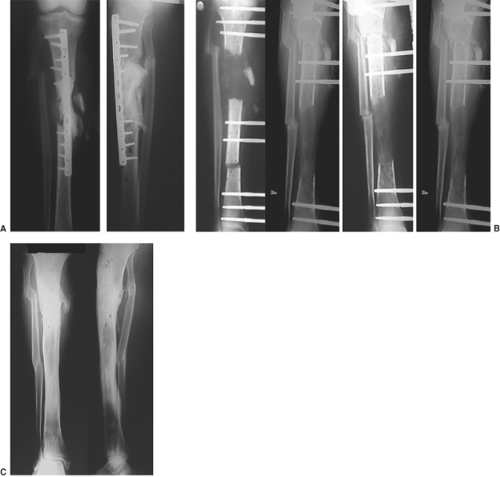 Figure 21.2. Example of a severely infected proximal tibial nonunion and loosened internal fixation (A). The patient underwent surgical osseous and soft tissue debridement and removal of hardware. This was followed by a distal tibial corticotomy and proximal transportation of a bone segment for the management of the severely proximal tibial bone loss (B). Note the use of a uniplane monolateral external fixator and final outcome (C). |
In a trifocal technique for the management of closed bone loss with one proximal and one distal corticotomy, the soft tissue issue can cause major obstacles for the completion of the procedure. When performing these corticotomies, the docking site will be at a level about the middle of the lower extremity. This procedure usually requires four clamps when using a monolateral external fixation system or four to five circular rings when using a circular external fixation system. The most proximal clamp or ring and the most distal clamp or ring will be fixed on the external fixation device, while the two clamps or rings in the middle will be transporting the necessary bone fragments. The proximal clamp or ring will move distally toward the midportion on the lower extremity while the distal one will move proximally in a similar fashion toward the midportion of the lower extremity. Regular skin releases throughout this process are necessary to avoid any postoperative complications (Figure 21.5).
Finally, both Schanz pins and/or smooth wires can create small wounds at the trailing side that usually heal by secondary intention. This is usually the most common site for pin or wire irritation and/or infection and great attention is given in order to avoid any further complication and possible removal. Extra
caution is considered in cases where an intramedullary nailing technique is used in combination with the circular external fixator for the bone transport in order to avoid any pin or wire site infection (Figure 21.6).
caution is considered in cases where an intramedullary nailing technique is used in combination with the circular external fixator for the bone transport in order to avoid any pin or wire site infection (Figure 21.6).
 Figure 21.3. Example of a trifocal technique in a 60-year-old diabetic patient with traumatic bone and soft tissue loss of the right proximal tibia (A). Two distal tibial corticotomies were performed with partial closure of the large wound proximally (B–D). Note the use of a uniplane monolateral external fixator to facilitate any plastic surgery procedures if needed. Final radiographic and clinical views (E, F) showing satisfactory regenerate bone distally, safe docking proximally, and complete soft tissue closure by distraction osteogenesis techniques.
Related posts: History and Evolution of External Fixation History and Evolution of External Fixation
 Stepwise Approach to Static Circular External Fixation Stepwise Approach to Static Circular External Fixation
 Stepwise Approach to Midfoot and Hindfoot Elective and Reconstructive Surgery with External Fixation Stepwise Approach to Midfoot and Hindfoot Elective and Reconstructive Surgery with External Fixation
 Stepwise Approach to Forefoot Elective and Reconstructive Surgery with External Fixation Stepwise Approach to Forefoot Elective and Reconstructive Surgery with External Fixation
 Stepwise Approach to Foot and Ankle Osteomyelitis and External Fixation Stepwise Approach to Foot and Ankle Osteomyelitis and External Fixation
 Surgical Off-loading External Fixation and Plastic Reconstruction of the Foot and Ankle Surgical Off-loading External Fixation and Plastic Reconstruction of the Foot and Ankle
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|