In the context of an important national congress and, when colleagues meet to discuss the latest developments in our field of interest, it is of relevance to reflect on the evolution and development of the medical specialty of physical and rehabilitation medicine (PRM). This reflection naturally includes a review of the past, an analysis of the present, and the necessary and inevitable speculation about the future. I had the privilege to share my thoughts on this topic with the 30th Congress of the Société française de médecine physique et de réadaptation held in Montpellier, France on October 8–10, 2015. This article is a summary of that presentation with some additional considerations.
1
Our core values
Disability is a unique human experience that contributes to human diversity and PRM is the only medical specialty whose main purpose is to understand disability in all its dimensions and to ameliorate its consequences by developing interventions to enhance function and improve quality of life.
The roots of modern PRM as a medical specialty can be traced back, at least, to the 19th century. Although we have witnessed many changes in the way PRM is understood and practiced some of the core values remain the same and have been briefly summarized recently by DeLisa as follows:
- •
enhancing function and independence is as important as finding a cure for a disease;
- •
physical agents (including exercise) can be as important as chemical agents;
- •
caregivers include not only the health care team but also the patient, his/her family, and friends;
- •
patient care is provided by a team;
- •
PRM professionals are obligated to change the patient’s environment and community;
- •
the multiple roles of PRM professionals include social advocacy.
By definition, core values are the essence of a profession and determine the course of action we select when given choices. As we plan and work for the future of PRM, it is important to always keep these core values in mind.
2
A profession and a medical specialty
By definition, a profession (and a medical specialty) is a calling or occupation requiring specialized knowledge and long and intensive preparation including instructions in skills and methods as well as in the scientific, historical, or scholarly principles underlying such skills and methods. It is worth considering what is the current status of both, knowledge and science in PRM, and how much progress we have made in both areas.
2.1
Knowledge content in PRM
I strongly believe that the quantity and the quality of our knowledge base have increased significantly in the last few decades. It has been said that when Charles II of England had a mild stroke, the treatment (and rehabilitation) administered by his personal physicians included bleeding, purgatives, enemas, sneezing powder, and antidotes containing extracts of herbs and animals . Needless to say, today’s protocols for the treatment and rehabilitation of stroke are vastly different. This is due to the considerable amount of new information and knowledge that has resulted from scientific research in rehabilitation. A quick search of articles registered in PubMed (a database of more than 25 million citations for biomedical literature from MEDLINE, life science journals, and online books) using the term “physical and rehabilitation medicine” shows that the number of published manuscripts in this field increased by a factor of 10 between the years 1975 and 2014. A similar search using the term “stroke rehabilitation” shows a 45 fold increase and a search for the term “exercise” shows an approximate 10-fold increase in the number of manuscripts published in the same time period.
It is also interesting to note that not only the amount of also the type and nature of the information included in some of the major textbooks in the specialty has changed dramatically. For example, a textbook published in the United States in 1982 included such topics as pre-vocational evaluation, massage, ultraviolet therapy, diathermy, bed positioning, training in homemaking activities, and footwear and footwear modifications. On the other hand, a recent textbook published in 2010 , emphasized topics such as imaging techniques, the application of the ICF in rehabilitation medicine, sports medicine, aging and rehabilitation, injection procedures, transplantation medicine, regenerative medicine, the conduct of clinical trials, and rehabilitation robotics. The topics in the former textbook have not disappeared completely from our field of study but have become less relevant in the modern practice of PRM. This shift in knowledge content and topics of interest is due in part to a more comprehensive approach to the process of rehabilitation and to the dramatic advances in medicine and science in general that have influenced the teaching and scope of practice of PRM.
2.2
Scientific research in PRM
Research that uses the scientific method is one of the best strategies available to humans who want to understand nature and the world. In the context of clinical medicine, scientific research is based on the use of sound study designs and the systematic search for evidence that could change the practice of a medical specialty and the treatments available for patients. In this regards, success will depend on the development of research capacity and a research agenda that is responsive to the needs of persons with disabilities . Capacity building is a process of individual and institutional development that leads to a higher level of skill and a greater ability to perform research . The elements of research capacity are briefly presented in Table 1 . Although few precise data on the current situation of research capacity in various countries have been published, an increase in both the number of scientific journals and publications in the field of PRM suggest that some of the elements of research capacity have been significantly enhanced in recent decades.
| Element | Comment |
|---|---|
| Researchers | A pool of well-qualified researchers with the appropriate training and mentoring, a strong commitment to inquiry, and desire to collaborate with others |
| Research culture, environment, and infrastructure | Recognition of research and scientific discovery as an institutional, organizational, and professional core value; needed human and physical resources |
| Partnerships | Partnerships with scientists in other disciplines, academic departments, institutions and with patient advocacy groups are vital to enhancing the capacity for conducting interdisciplinary, high-quality, meaningful research |
| Funding | Generous budgets dedicated to scientific research with an emphasis on rehabilitation medicine; funding for different stages of a scientific career |
| Metrics | Indicators of success |
On the other hand, a research agenda represents an outline or list of questions and areas of scientific inquiry relevant to the specialty. This agenda should incorporate all levels of the clinical and translational research continuum including basic, human clinical, practice-based, and global health research. A quick overview of recent publications in PRM show that researchers are targeting all four levels of the continuum including basic research questions using animal and in vitro models, human clinical trials, practice-based research including outcomes and health services research, and population health studies. This comprehensive approach is required in PRM because of the broad spectrum of health conditions that require and could benefit from rehabilitative interventions.
2.3
Clinical trials in PRM
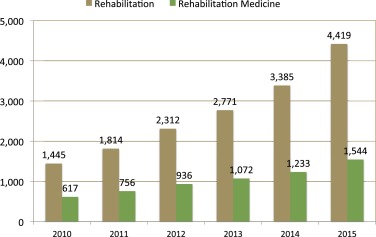
One of the most widely accepted research study design for the generation of new knowledge for use in human populations is the randomized controlled trial (RCT). A clinical trial is defined as “any research study that prospectively assigns human participants or groups of humans to one or more health-related interventions to evaluate the effects on health outcomes.” ( http://www.who.int/ictrp/en ). The total number of randomized controlled trials (> 200,000 in December, 2015) in all categories in 191 countries of the world officially registered in one database ( http://www.clinicaltrials.gov/ ) has increased significantly in the last 5 years ( Fig. 1 ). More relevant to this commentary, in the “rehabilitation” category, the number of trials has increased from 1445 in 2010 to 4412 active registered trials in the month of December, 2015. This volume of RCT’s is very similar to the number of RCT’s in closely related specialties such as neurosurgery, neurology, and orthopedics. Because many considered RCT’s the gold standard by which the quality of scientific evidence should be judged, this increase in RCT’s in PRM has to be considered a very positive development. Several PRM journals have published a larger number of RCT’s in the last few years including a recent special issue of the American Journal of Physical and Rehabilitation Medicine dedicated to RCT’s published in October 2015.
Related posts:
 Effect of submental sensitive transcutaneous electrical stimulation on virtual lesions of the oropharyngeal cortex
Effect of submental sensitive transcutaneous electrical stimulation on virtual lesions of the oropharyngeal cortex
 Contribution of isokinetic muscle strengthening in the rehabilitation of obese subjects
Barriers to home-based exercise program adherence with chronic low back pain: Patient expectations regarding new technologies
Intermittent catheterization in neurologic patients: Update on genitourinary tract infection and urethral trauma
Contribution of isokinetic muscle strengthening in the rehabilitation of obese subjects
Barriers to home-based exercise program adherence with chronic low back pain: Patient expectations regarding new technologies
Intermittent catheterization in neurologic patients: Update on genitourinary tract infection and urethral trauma
 Muscle strengthening for hemiparesis after stroke: A meta-analysis
Muscle strengthening for hemiparesis after stroke: A meta-analysis
 A comprehensive picture of 4-year outcome of severe brain injuries. Results from the PariS-TBI study
A comprehensive picture of 4-year outcome of severe brain injuries. Results from the PariS-TBI study
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


