Single Ventricle
Edward V. Colvin
A univentricular atrioventricular (AV) connection is present when both atria are connected to a single chamber within the ventricular mass. Even though most hearts so constituted have two chambers within the ventricular mass, single ventricle is the term used most often for this anomaly.
NOMENCLATURE
The segmental approach to nomenclature is used to describe single-ventricle hearts (Fig. 268.1). This nomenclature is presented in Box 268.1.
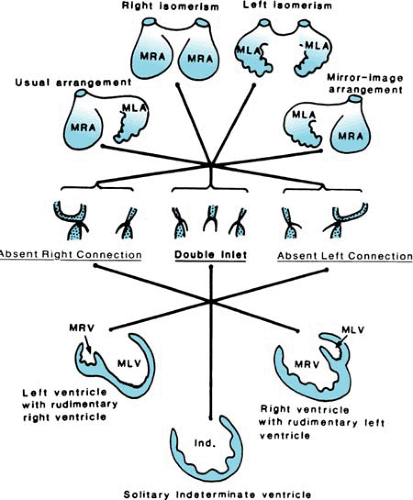 FIGURE 268.1. Atrial situs, modes of atrioventricular connection, and types of ventricular morphology. LA, left atrium; LV, left ventricle; M, morphologic; RA, right atrium; RV, right ventricle. (Reprinted from Becker AE, Anderson RH, Penkoske PA, Zuberbuhler JR. Morphology of double inlet ventricle. In: Anderson RH, Crupi G, Parenzan L, eds. Double inlet ventricle. Tunbridge Wells, UK: Castle House Publications, 1987:36, with permission.) |
ANATOMY
Hearts with univentricular AV connection are subdivided according to ventricular morphology into three basic types: dominant left, dominant right, or indeterminate ventricular morphology. Dominant left or dominant right ventricular morphology can occur with D-loop or L-loop (Fig. 268.2).
The most common type is called double-inlet left ventricle, or single left ventricle. Usually, the nondominant ventricle is located anteriorly and to the left and gives rise to one or both of the great vessels.
Hearts in which the dominant chamber possesses an apical trabecular portion of right ventricular type are called double-inlet right ventricle, or single right ventricle. The nondominant ventricle is located posteriorly. Usually, this chamber has neither inlet nor outlet components.
Hearts in which only one abnormally trabeculated ventricle is found are termed hearts with univentricular AV connection and indeterminate ventricular morphology, or single-ventricle with morphologically undetermined myocardium.
Certain hearts have been described as having a ventricular mass containing a trabecular pattern typical of a right ventricle on one side and of a left ventricle on the other, with only a tiny
rim of apical ventricular septum. These hearts have a biventricular AV connection with a large ventricular septal defect.
rim of apical ventricular septum. These hearts have a biventricular AV connection with a large ventricular septal defect.
BOX 268.1. Terms Used to Describe Single-Ventricle Hearts
Atrial situs may be solitus, inversus, or ambiguus with bilateral right or left morphology. The type of atrioventricular (AV) connection is, by definition, univentricular. The mode of connection may be double-inlet, absent left, or absent right AV connection. In double-inlet connection, the two atria may be connected to the ventricle by two separate AV valves or via a common valve. Usually, the two AV valves do not have typical characteristics of mitral and tricuspid valves and therefore are termed right and left on the basis of the anatomic location of the atrium to which they are connected.
In descriptive morphologic terms, a complete ventricle may have inlet, apical trabecular, and outlet components. Usually, the apical trabecular portion can be used to classify a chamber as being of right or left morphology. In the morphologically right ventricle, the apical component has characteristic coarse trabeculations. In contrast, the apical component of the morphologically left ventricle has much finer crisscrossing trabeculations and a smooth septal surface.
When two chambers are found within the ventricular mass, one has a right and the other a left ventricular apical trabecular component. Usually, the ventricle receiving the AV valve or valves is larger and is termed the dominant ventricle. The other ventricle is described as nondominant, or rudimentary. Usually, the nondominant ventricle is small, but size varies. Outlet chamber and trabecular pouch describe a nondominant ventricle with and without an outlet component, respectively.
The spatial relation of the two ventricles is an important variable and must be specified. It has been designated by various authors as D– or L-loop, right– or left-hand ventricular architecture, and noninverted or inverted ventricles. When two ventricles are present, the communication between them properly is termed a ventricular septal defect (VSD). The terms outlet foramen and bulboventricular foramen also have been used to describe the VSD.
If two great vessels are present, the ventriculoarterial connection may be concordant, discordant, or double-outlet. A single-outlet connection may be present with a common arterial trunk or with aortic or pulmonary atresia.
INCIDENCE
Single ventricle is found in approximately 1% of children with congenital heart defects. Whereas most patients have no chromosomal abnormality, case reports document occasional association. Occurrence in siblings has been reported. Of 237 hearts in one series, 140 had a dominant left ventricle, 34 had a dominant right ventricle, and 41 had indeterminate morphology. Associated cardiovascular anomalies are common.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


