Reorganized Motor and Sensorimotor Control in Whiplash: Implications for Training
Deborah Falla
Gwendolen Jull
Whiplash-associated disorders (WAD) are a significant public health problem. Approximately 50% of those affected report persistent disability more than 1 year after the injury, resulting in both substantial personal and societal costs [4]. Moreover, up to 30% of those affected will remain moderately to severely disabled. The physical and psychological features associated with WAD are diverse, and various factors may contribute to the chronicity of symptoms. Here, the focus is on the motor and sensorimotor adaptations that may occur following a whiplash injury. Moreover, the implications of these findings for the rehabilitation of people with WAD are discussed.
Individuals who have suffered a whiplash injury typically present with some degree of impaired motor function such as reduced neck strength, which may be apparent around all axes, and/or reduced force steadiness. Range of motion is also usually restricted and, in general,
people with neck pain may show increased range of motion variability, decreased movement speed, and reduced smoothness of neck movement (for review see [17]).
people with neck pain may show increased range of motion variability, decreased movement speed, and reduced smoothness of neck movement (for review see [17]).
Although pain can impair motor output, several studies have shown that in the presence of goal-oriented submaximal tasks, the kinematic output may be unchanged [15]. Muscular adaptation occurs (i.e., redistribution of the activity within the same muscle or across synergistic muscles) to maintain unaltered motor output but with modified muscle load. Accordingly, changes in muscle activation and muscle coordination are well documented in people with whiplash-induced neck pain and are largely similar to the changes observed in people with insidious-onset neck pain. Such changes may include reduced activation of the deep cervical flexors (longus colli, longus capitis) during performance of brief isometric craniocervical flexion contractions [9] or delayed activation of these muscles when exposed to rapid postural perturbations [8]. Poorer control of the deep cervical flexor muscles is associated with increased activation (likely compensatory) of the sternocleidomastoid and anterior scalene muscles [9], an observation that has been documented within the first 4 weeks of a whiplash injury [32]. More recent work also showed reduced activation of the deep extensor muscle, semispinalis cervicis, in people with trauma-induced neck pain [30], reinforcing the frequent observation of impaired activation of the deeper spinal muscles in people with spinal pain disorders.
Reduced specificity of neck muscle activation is another feature of altered motor control of the neck observed in people with chronic neck pain disorders [12, 30] (Fig. 4-1). A loss of the predefined patterns of muscle activation has been noted for several neck muscles (e.g., sternocleidomastoid, splenius capitis, semispinalis cervicis) in several patient groups (e.g., WAD, idiopathic neck pain) and supports the relatively consistent finding of augmented activity of the superficial muscles in people with neck pain disorders, regardless of the task examined; for example, cervical flexion, craniocervical flexion, and movements of the upper limb. Increased coactivation of the neck flexor and extensor muscles may also be present, and is inversely correlated with total neck strength and positively correlated with levels of pain and perceived disability [23]. High levels of neck muscle coactivation may reflect an
attempt to voluntarily increase the stability of the head/neck for the fear of performing potentially painful movements. This fits with the contemporary theory that sensorimotor adaptation to pain has a general aim (at least in the short term) to protect the painful/threatened body part from real or anticipated further pain/injury [16].
attempt to voluntarily increase the stability of the head/neck for the fear of performing potentially painful movements. This fits with the contemporary theory that sensorimotor adaptation to pain has a general aim (at least in the short term) to protect the painful/threatened body part from real or anticipated further pain/injury [16].
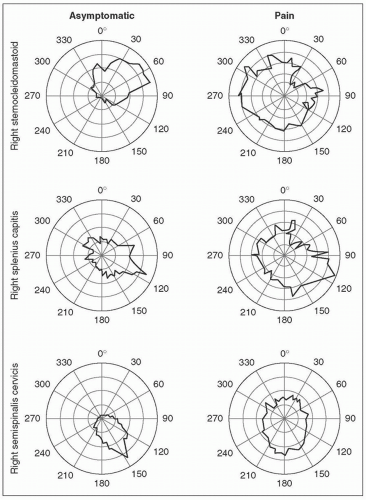 FIGURE 4-1 Representative directional activation curves obtained from the sternocleidomastoid, splenius capitis and semispinalis cervicis muscles during a circular contraction performed at 15 Newtons presented for a control subject and a patient with chronic neck pain. Note the defined activation of the sternocleidomastoid, splenius capitis, and semispinalis cervicis for the control subject with minimal activity during the anatagonist phase of the task. Conversely, the directional activation curves for the patient indicate more even activation levels of each muscle for all directions resulting in increased coactivation of the neck flexor and extensor muscles. (Reprinted with permission from Falla et al. [12], Lindstrøm et al. [23] and Schomacher et al. [30].) |
Recent work has revealed that during repetitive arm movements, load sharing between neck muscles, as seen in asymptomatic people, is reduced in people with WAD. That is, people with WAD showed less variability in the pattern of neck muscle activation throughout the repetitive task [29]. Decreased motor variability during repetitive work has also been reported in people with chronic neck-shoulder pain and may result in higher fatigue and pain. Studies in patients with trapezius myalgia show similar results. For example, patients with trapezius myalgia activate the same region of the upper trapezius muscle continuously throughout a sustained shoulder abduction contraction, whereas asymptomatic subjects show redistribution of muscle activity across the duration of the contraction, resulting in less muscle fatigue [6].
Whiplash-induced pain has also been associated with a number of sensorimotor adaptations including impaired proprioception, reduced postural stability, and reduced smoothness of eye movements. Greater errors in positioning the head following voluntary movement have been shown in persons with neck pain of both insidious and traumatic onset, but proprioceptive acuity appears to be more affected in people with chronic whiplash especially in those reporting higher pain and disability and dizziness [34]. In addition to greater repositioning errors with head movement, some people with WAD show reduced proprioception at the shoulder and elbow that could affect the coordination and movement of their upper limb. Disturbed postural stability includes larger postural trunk sway both in stance tasks and in complex tasks such as walking up and down stairs, and reduced head stability in response to predictable and unpredictable postural perturbations [25]. Consistent with observations for head relocation accuracy, people with whiplash-induced pain generally show greater disturbances compared to patients with idiopathic neck pain, and postural instability is positively associated with the symptom of
dizziness [34]. Changes in oculomotor control have also been demonstrated in people with whiplash, suggestive of disturbances in the cervicocollic and cervico-ocular reflexes [34].
dizziness [34]. Changes in oculomotor control have also been demonstrated in people with whiplash, suggestive of disturbances in the cervicocollic and cervico-ocular reflexes [34].
Variability of Motor and Sensorimotor Adaptations
As reviewed above, people with WAD may present with many motor and/or sensorimotor adaptations (Fig. 4-2). However, it is well known that people with WAD form a heterogeneous group in terms of the associated pain mechanisms, psychological features, and physical signs. In relation to the type and extent of neuromuscular adaptations observed in people with WAD, there is substantial variability between individual patients. This variability likely relates to interactions between the nature and extent of the injury, the magnitude of pain and disability, and the
presence and magnitude of attendant stress reactions. Some evidence supports the premise that variability is partially related to the magnitude of pain. For example, augmented sternocleidomastoid and anterior scalene muscle activity during repetitive arm movements is greatest in patients reporting higher levels of pain and disability [7]. Furthermore, higher levels of pain are associated with greater delays in the activation of the deep cervical flexors during rapid flexion of the shoulder and lower amplitude of activation during isometric craniocervical flexion [13].
presence and magnitude of attendant stress reactions. Some evidence supports the premise that variability is partially related to the magnitude of pain. For example, augmented sternocleidomastoid and anterior scalene muscle activity during repetitive arm movements is greatest in patients reporting higher levels of pain and disability [7]. Furthermore, higher levels of pain are associated with greater delays in the activation of the deep cervical flexors during rapid flexion of the shoulder and lower amplitude of activation during isometric craniocervical flexion [13].
 FIGURE 4-2 People with whiplash-associated disorders (WAD) may present with many motor and sensorimotor disturbances that may include, but that are not limited to, those presented here. |
We recently examined the effects of experimentally induced neck muscle pain on multimuscle control of neck movements during an aiming task [15]. A general decrease in the electromyography (EMG) amplitude was observed in the injected muscle together with redistribution (decrease/increase) of the activation of other muscles, in a subject-specific manner. Thus, this work showed that people tend to adopt an individual control strategy so that a painful stimulus in the neck triggers a subject-specific redistribution of neck muscular activation (Fig. 4-3). These findings support the proposal of a heterogeneous adaptation of motor control in response to pain [16].
Similar to motor adaptations, sensorimotor disturbances are variable between people with WAD in both the nature of impairments and their frequency of presentation [34]. All or any one combination of disturbances in proprioception, balance, and oculomotor control may present in the individual.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


