Reflex and Long Latency
Blink Responses
General
Electrical stimulation of the supraorbital nerve, a sensory branch of the trigeminal nerve, elicits the blink reflex response, which consists of two separate components: an early R1 and a late R2. Visual and auditory stimuli give a response with only one component. Whereas R1 is evoked only on the side of electrical stimulation, R2 is recorded bilaterally with unilateral electrical stimulation. The patient is either positioned in an armchair, relaxed, and with the eyes half-closed, or placed in a warm room, supine, and with eyes gently closed.
Recording Electrode Placements
E1 The active surface electrode is placed on the belly of the orbicularis oculi below the canthus. To pick up consensual R2 on a second channel, a second pickup (E1) is attached to the opposite orbicularis oculi muscle. A second ground is not needed.
E2 The reference electrode is placed on the side of the nose.
Ground
The ground is placed on the forehead or cheek.
Stimulation
(Fig. 7-1, Fig. 7-2) Electrical stimulation is applied over the supraorbital nerve, which is in the groove that is palpable at the medial third of the superior orbit, with the cathode placed over the supraorbital foramen. The infraorbital or mental nerve can be used instead of the supraorbital. Stimulation intensity is usually 3 to
8 milliamperes (mA) (up to 16 to 20 mA), with duration of stimulus between 0.1 and 1 msec. Stimulus of low intensity causes the second response of the blink reflex to have a prolonged latency. Thus, it is necessary to determine the stimulus intensity that will evoke the maximum R2 amplitude. With better stimulus control, there is less variability and more reproducibility of responses.
8 milliamperes (mA) (up to 16 to 20 mA), with duration of stimulus between 0.1 and 1 msec. Stimulus of low intensity causes the second response of the blink reflex to have a prolonged latency. Thus, it is necessary to determine the stimulus intensity that will evoke the maximum R2 amplitude. With better stimulus control, there is less variability and more reproducibility of responses.
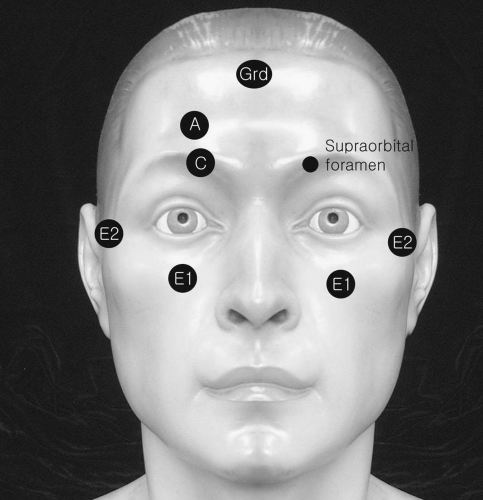 Figure 7-1. Placement of electrodes and stimulators for blink responses. |
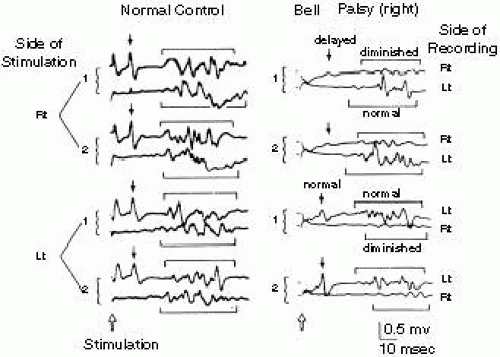 Figure 7-2. Two right-sided and two left-sided stimulations were delivered in each case to show consistency. In the patient, R1 (arrows) and R2 (single brackets) were delayed and small on the right side and normal on the left side regardless of the side stimulated. This finding indicates a lesion involving the efferent arc of reflex (facial nerve) on the right side. (Kimura et al.2) |
Electromyograph Settings
Reference Values
N = 83 normal adults, supraorbital nerve stimulation
R1 Component Latency
10.6 ± 2.5 ms [mean + 3 standard deviations (SD)]. It is delayed if it exceeds 13.0 ms. In normal patients, the difference between values for R1 on each side is less than 1.2 ms. Because R1 appears only ipsilaterally, to compare right with left, both sides must be stimulated. Reflex latency is measured from the stimulus artifact to the initial deflection of the evoked potential.
R2 Component Latency
Direct R2 (ipsilateral to the side of stimulus) is 31 ± 10 ms (mean + 3 SD). It is delayed if it exceeds 40 ms. The reflex latency is measured from the stimulus artifact to initial deflection of the potential. Consensual R2 latency (contralateral to the side of stimulus) is 32 ± 11 ms (mean + 3 SD). It is delayed if it exceeds 41 ms. The difference between values for R2 consensual and R2 direct is normally less than 5 ms (mean + 3 SD). This measurement requires only “one” stimulus, because R2 appears ipsilaterally and contralaterally to the side stimulated.
Neonates
N = 30
The contralateral R1 often is absent. It was bilaterally absent in one-third and usually ipsilateral only in the other two-thirds.
Comments
R1 usually is a biphasaic or triphasic wave (occasionally polyphasic). It tends to habituate slowly and is a brief, relatively synchronous reflex. It is more stable with repeated trials and better suited for assessing nerve conduction of the trigeminal and facial nerves.
Latency is measured from the stimulus artifact to the initial deflection of the evoked potential (R1 or R1). Kimura1 suggests using the shortest latency of eight stimulations.
Both R1 and R2 waves probably are due to a polysynapatic brain stem reflex, the blink reflex, with the afferent arc provided by the sensory branches of the trigeminal nerve and the efferent arc provided by the facial nerve motor fibers.
R1 is affected by lesions in:
trigeminal nerve (afferent arc)
pons (central arc)
facial nerve (efferent arc)
R2 is affected by:
level of consciousness
lateral medullary lesion
contralateral hemispheric lesion
parkinsonism
medication [diazepam (Valium)]
When the supraorbital nerve is stimulated, both R1 and R2 are regularly elicited in normal patients.
When the infraorbital nerve is stimulated, R2 is always present, but R1 is inconsistent in normal patients.
When the mental nerve is stimulated, R2 is inconsistent, and R1 is present only rarely in normal patients.
H Reflex Latency to the Gastrocnemius
(Fig. 7-3)
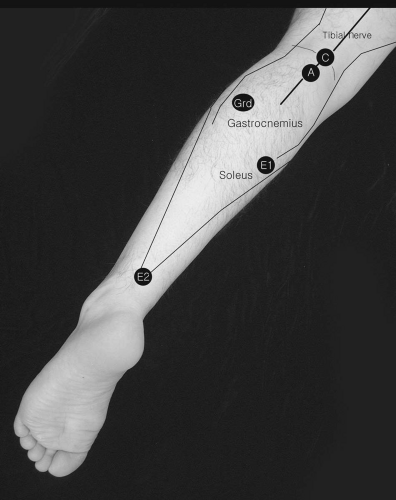 Figure 7-3. H reflex recording from either soleus or gastrocnemius muscle. |
Braddom’s Technique4
E1 The patient is prone with the feet suspended over the edge of the table or with a pillow placed under the ankle. The E1 active electrode is placed on the bisecting point of a line connecting the popliteal crease and the proximal flare of the medial malleolus.
E2 The reference electrode is attached over the Achilles tendon.
Electromyography Machine Settings
Stimulation
Percutaneous stimulus with low-intensity current (submaximal stimulus) is used. The stimulation pulses of long duration (i.e., 0.5 to 1 ms) are used to preferentially activate a large diameter of sensory fibers. The cathode is proximal and is placed over the tibial nerve in the popliteal fossa at the level of the popliteal crease. The H waves are more easily recorded with the muscle at rest, although contraction of the recording muscle may enhance the H reflexes. Placing an anode over the patella may avoid a large stimulus artifact.
Reference Values
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


